Download
1 / 64
660 likes | 1.38k Views
Jaundice. Medical Audience Attention Span. 1.0= Normal Vigilance. In Tens of Minutes. Overview. What is “jaundice”? Types Etiologies Diagnosis. What is jaundice?. The french word jaune - yellow. Icterus - yellowish discoloration Skin, conjunctiva, sclera, mucous membranes

E N D
Medical Audience Attention Span 1.0= Normal Vigilance In Tens of Minutes
Overview • What is “jaundice”? • Types • Etiologies • Diagnosis
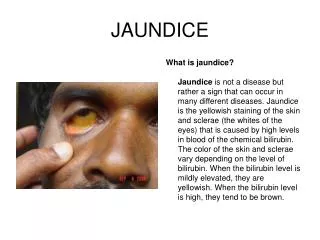
What is jaundice? • The french word jaune - yellow. • Icterus - yellowish discoloration • Skin, conjunctiva, sclera, mucous membranes • Appears 'top to bottom' (face to feet) • Resolves 'bottom to top'.
Technical definition • Hyperbilirubinemia • Normal less than 1.2 mg/ml • Less than 5 percent conjugated • Not visual until greater than 2.5 mg/ml • Best seen in sclera and oral mucous membranes (look at soft palate)
RBC destruction Hemoglobin degraded to heme Spleen turns into unconjugated bilirubin Transported to liver Conjugated with glucuronic acid Passed into bile Small bowel bacteria convert to stercobilinogen Oxidised to stercobilin. Some reabsorbed, excreted renally as urobilinogen Oxidised into urobilin Bilirubin
A Tale of Two Hyperbilirubinemias • Unconjugated • Overproduction • Impaired uptake • Conjugation abnormalities • Mixed • Hepatocellular disease • Impaired canalicular excretion • Obstruction
Or… • Pre-hepatic or hemolytic causes • Hemolysis • Hepatic causes • Conjugation problems • Post-hepatic or extrahepatic • Excretion of bile disrupted
Unconjugated Hyperbilirubinemia • Overproduction • Hemolysis • Extravascular vs intravascular • Extravasation • Dyserythropoiesis • Reduced hepatic uptake • Impaired conjugation • Physiologic jaundice of newborn • Consists of all three
Overproduction • Normal liver can keep up • Bilirubin < 4-5 mg/dl • Conjugated bilirubin remains 3-5 percent • Hepatic disease affects canilicular excretion • Bilirubin diffuses back into plasma
Conjugation Function • Gilbert’s • Crigler-Najjar
What about Gilbert? • Reduced levels of Uridinediphosphoglucuronate glucuronosyltransferases (UGTs) • Mutation in the promoter region • Deficiency in isoform that conjugates bilirubin to glucuronic acid • Creates a backflow equilibrium
And Crigler-Najjar? • Type I - UGT with no activity • Kernicterus • Fatal without liver transplant • Type II – UGT with reduced activity • Less severe than type I
Are you new here? • Conjugating activity low in neonates • Turn over of fetohemoglobin to adult forms • May need light therapy
Other Effects on Activity • Decreased UGT activity • Antibiotics • Hepatitis • Chronic hepatitis • Advanced cirrhosis • Wilson’s disease • Hyperthyroidism • Ethinyl Estradiol • Increased activity • Progestational and estrogenic steroids
Conjugated Hyperbilirubinemia • Intrahepatic cholestasis • Extrahepatic cholestasis/obstruction • Hepatocellular injury
Dubin-Johnson • Autosomal recessive • Human canalicular multispecific organic anion transporter (cMOAT) mutation (multidrug resistance protein 2 (MRP2)) • Impaired transport • Accumulation of hepatocellular pigment. • Rare, Sephardic Jews • Prevalence 1:1300. • Life expectancy normal • Reduced prothrombin and factor VII activity • Nonpruritic jaundice in teenage years.
Rotor Syndrome • Rare, Autosomal Recessive • Mechanism not clear • chronic mixed hyperbilirubinemia • Storage defect • Benign • Labs and histology normal • Biopsy not required • Urinary coproporphyrin 250 to 500% normal, 65% coproporphyrin I • Dubin-Johnson syndrome - urinary coproporphyrin normal, 80% coproporphyrin I • Normal – urinary porphyrins 75% coproporphyrin III
Obstruction • Bilirubin retained • Glucuronidation reversed • Unconjugated bilirubin diffuses into plasma • Mixed bilirubin transported into plasma by MRP transporters.
Differential Dx • Cholelithiasis • Tumors • Primary sclerosing cholangitis • Parasites • Pancreatitis • Strictures (benign/malignant) • AIDS cholangiopathy
AIDS Cholangiopathy • Cryptosporidium • CMV • HIV • Biopsies or bile cultures for dx
Viral Hepatitis HSV EBV Tumors Lymphoma Kaposi’s Drugs Mycobacterium TB Atypical mycobacterium Fungi Cryptococcus Histoplasma Candida Coccidioides Pneumocystis carinii Other HIV Possibilities
Intrahepatic Cholestasis • Jaundice • Bile ducts are patent
Viral Hepatitis Alcoholic Hepatitis Non-Alcoholic Steatohepatitis Primary Biliary Cirrhosis Drugs Toxins End-stage liver disease Sepsis Low perfusion states Malignancy Liver infiltration TPN Post-operative Post-transplant Sickle Cell disease Pregnancy Etiologies
Alcoholic Hepatitis • Cholestasis • Fever • Leukocytosis • History of EtOH • AST to ALT exceeds 2.0 • AST and ALT each less than 500
Similar to EtOH but NO EtOH Obesity DM Female Amiodarone Antiviral drugs (nucleoside analogues) Aspirin / NSAIDS Statins Corticosteroids Methotrexate Nifedipine Perhexiline Tamoxifen Tetracycline Valproic acid NASH
PBC • Cholestatic and hepatocellular injury picture • Antimitochondrial antibodies • Present in 95 percent • 95 percent sensitive, 98 percent specific • Anti-nuclear antibodies • In 70 percent of patients
Drugs • Dose related • Allergic reactions • Idiosyncratic • Mixed hepatocellular/cholestatic picture • Thorough drug history imperative
Low Perfusion States • Sepsis • Hyperbilirubinemia can promote sepsis • CHF • Hypotension • Hypoxemia
Paraneoplastic Syndromes • Stauffer’s Syndrome • Uncommon in RCC • Absence of metastases • Cholestasis, elevated alkaline phosphatase. • Fever • Weight loss • Fatigue • Poor prognosis • Related to tumor cytokines • Nephrectomy may ameliorate • Recurrence - maybe more cancer or metastases
Infiltration • Amyloidosis • Sarcoidosis • Lymphoma • TB
TPN • Steatosis • Lipidosis • Cholestasis (after 2-3 weeks of Rx) • Bacterial overgrowth
Multifactorial Transfusions Hematomas Hemolysis Sepsis TPN Drugs (anesthetics) Hypoxia Hypotension Viral Hepatitis Renal Failure Post Operative
Bone Marrow and Liver mostly TPN Drugs Immunosuppressives Radiation Chemotherapy Graft rejection Preservation injury Operative complications Post Transplant
Sickle Cell Disease • Chronic hemolysis • Hepatic dysfunction • Cirrhosis • Secondary hemochromatosis • Hepatic crisis • Hepatomegaly and tenderness • Severe hyperbilirubinemia • Bilirubin microliths, sludge, stones common • Obstruction rare
Intrahepatic Cholestasis of Pregnancy (IHCP) • Third Trimester • Possibly genetic • Pruritus >> cholestasis >> Jaundice • Maybe more premature/still births • Distinguish from acute fatty liver and HELLP
Acute Fatty Liver of Pregnancy • microvesicular fatty infiltration of hepatocytes • 1 in 7000 to 1 in 16000 deliveries • Second half of pregnancy, usually third trimester • Nausea, vomiting, abdominal pain, anorexia, and jaundice, preeclampsia • Delivery is curative (and mandatory!)
HELLP • Hemolysis, Elevated Liver enzymes, Low Platelets • 1 of 1000 pregnancies • 10 to 20 percent with preeclampsia or eclampsia • Diagnosed between 28 and 36 weeks of gestation • 70 percent occurred prior to delivery • Delivery is mandatory!
End Stage Liver Disease • Supportive Care • Transplant
Hepatocellular Injury • Neoplasms • Viral • Bacterial • Congenital • Parasitic • Fungal • Systemic • Immunologic • Toxic
Viral • Hepatitis A, B, C, D, E • HSV • Hemorrhagic viruses • Adenoviruses • Enteroviruses
Bacterial • TB • Leptospirosis • Syphilis • Brucella • Rickettsia • Tropheryma Whippelii • Rochalimea