Download
1 / 43
550 likes | 1.22k Views
Jaundice. Dr. Firas Obeidat , MD. Bilirubin metabolism. Bilirubin metabolism. What causes bilirubin ? overproduction by reticuloendothelial system. failure of hepatocyte uptake. failure to conjugate or excrete. obstruction of biliary excretion into intestine.

E N D
Jaundice Dr. FirasObeidat, MD
Bilirubin metabolism • What causes bilirubin? • overproduction by reticuloendothelial system. • failure of hepatocyte uptake. • failure to conjugate or excrete. • obstruction of biliary excretion into intestine.
Prehepatic (hemolytic) jaundice • Excessive production of bilirubin. • Ability of the liver to conjugate is overcame. • Increase plasma unconjugated bilirubin.
Intrahepatic jaundice • Defect may be in: • uptake. • conjugation. • secretion. • Reflects liver dysfunction. • In addition to high bili, biochemical liver markers are high.
Posthepatic jaundice • Secondary to biliary obstruction. • Increase of conjugated bilirubin. • GGT, ALP • Clinical: • pale colored stool (absence of fecal bilirubin ) • dark urine ( increased conjugated bilirubin ) • itching
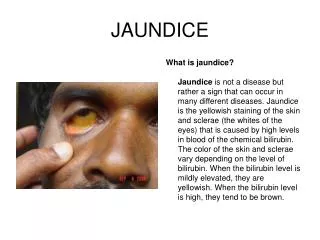
Approach to the Jaundiced Patient • Definition. • Imbalance between bili production and excretion appears as jaundice. • The appearance of jaundice also depends on: • which type of bilirubin is elevated. • duration.
Clinical Evaluation and Investigative Studies • History and physical examination: • examine the mucous membranes of the mouth, the palms, the soles, and the sclerae in natural light. • Why? • protected areas from photodegradation • skin will be the only site of coloration due to consumption of large quantities of food containing lycopene or carotene or drugs such as rifampin. careful inspection of elastic tissues reveal no jaundice.
Clinical Evaluation and Investigative Studies • Direct versus indirect hyperbilirubinemia: • ask about urine and stool color. • pruritus. • look for scratch marks. • rarely, the clinical picture may be secondary to a massive increase in both direct and indirect bilirubin production.
Causes of UnconjugatedHyperbilirubinemia • Increased RBC breakdown: • acute hemolysis. • chronic hemolytic disorders. • large hematoma resorption, multiple blood transfusions. • Gilbert syndrome. • Decreased hepatic bilirubin conjugation: • Gilbert syndrome. • Familial unconjugatedhyperbilirubinemia.
Unconjugated (Indirect) Bilirubin • In case of hemolysis: • excissive production of unconjugated bilirubin. • normal liver will handle extrabilirubin. • slight rise in serum levels is observed. • Blood tests reveal that 60% to 85% of bilirubin is indirect.
Unconjugated (Indirect) Bilirubin • The diagnosis of indirect hyperbilirubinemia attributable to hemolysis is confirmed by: • elevated serum (LDH) level (abundant in RBCs). • decreased serum haptoglobin level. • evidence of hemolysis on microscopic examination of the blood smear.
Unconjugated (Indirect) Bilirubin • In case of decreased hepatic bilirubin conjugation: • Gilbert syndrome, is the most common: • benign condition affecting up to 7% of the population. • characterized by a defect in glucuronyltransferase I gene. • impairment of bilirubinglucuronidation • affected patients may have jaundice after stress or infection.
Cholestatic Syndrome • conjugated hyperbilirubinemia: • hepatic jaundice (nonobstructive or medical jaundice) due to defect in hepatocellular function. • posthepatic jaundice (obstructive or surgical jaundice ) as a result of blockage somewhere in the biliary tree.
Cholestatic Syndrome • characteristics: • conjugated hyperbili. (dark urine, pale stools, pruritus ). • chronic malabsorption of fat-soluble vitamins.
HEPATIC VERSUS POSTHEPATIC JAUNDICE • After confirmation of the presence of direct hyperbilirubinemia, the next step is to determine whether the jaundice is hepatic or posthepatic. • The sensitivities of history, physical examination, and blood tests alone range from 70% to 95. • The overall accuracy : 87% to 97%.
HEPATIC VERSUS POSTHEPATIC JAUNDICE • Clinical manifestations: • hepatic jaundice: • acute hepatitis. • a history of alcohol abuse. • physical findings reflecting cirrhosis or portal hypertension. • posthepatic jaundice: • abdominal pain. • rigors, itching. • hepatomegaly. • patients are usually younger.
HEPATIC VERSUS POSTHEPATIC JAUNDICE • Summary: • clinical approach supported by simple biochemical evaluation displays good predictive ability to distinguish hepatic from posthepatic jaundice. • clinical approach alone does not accurately identify the level of biliary obstruction in a patient with posthepatic jaundice.
Causes of Hepatic Jaundice • Hepatitis (viral, autoimmune or alcoholic). • Drugs and hormones. • Diseases of intrahepatic bile ducts. • Liver infiltration and storage disorders. • Systemic infections. • Total parenteral nutrition. • Postoperative intrahepaticcholestasis. • Cholestasis of pregnancy. • Benign recurrent intrahepaticcholestasis. • Infantile cholestatic syndromes. • Inherited metabolic defects. • No identifiable cause (idiopathic hepatic jaundice).
Hepatic Jaundice • Hepatic jaundice may be either acute or chronic. • Acute hepatic jaundice: • de novo or in the setting of ongoing liver disease. • Causes: medications or viral hepatitis. • Physical examination usually reveals little. • treatment in most cases remains supportive.
Hepatic Jaundice • Chronic hepatic jaundice: • patient may have chronic hepatitis, with or without cirrhosis. • causes : viral infection, drug, autoimmune liver disease. • Physical examination: stigmata of chronic liver disease. • Treatment: supportive. • to quantify hepatic reserve: Child-Pugh classification. • end-stage liver disease: liver transplantation.
(MELD) score • The Model for End-Stage Liver Disease . • the most accepted score for allocation of organs for liver transplantation. • This score is based on: • serum bilirubin. • creatinine concentrations. • international normalized ratio (INR). • No subjective components of the Child-Pugh score (e.g., ascites and encephalopathy).
IMAGING • It is the next step after Hx, physical examination and laboratory assessment. • Goals: • to confirm the presence of an extrahepatic obstruction. • to determine the level of the obstruction. • to identify the specific cause of the obstruction. • staging information in cases of malignancy).
IMAGING • Direct cholangiography (ERCP, PTC): gold standard for defining the level of a biliary obstruction. • Ultrasonography: ductal dilatation with or w/o GB distension, presence of liver causes. • MRCP , CT scan and EUS: location and nature of biliary obstruction. Diagnosis and staging biliopancreatic tumors.
Workup and Management of Posthepatic Jaundice • Once ultrasonography has confirmed that ductal obstruction is present, there are three possible clinical scenarios: • suspected cholangitis. • suspected choledocholithiasis without cholangitis. • suspected lesion other than choledocholithiasis.
Workup and Management of Posthepatic Jaundice • suspected cholangitis: • presence of (Charcot's triad or Raynaud's pentad), the most likely diagnosis is choledocholithiasis. • ERCP is indicated for diagnosis and treatment. • Antibiotics with adequate biliary drainage is the mainstay of treatment .
Workup and Management of Posthepatic Jaundice • SUSPECTED CHOLEDOCHOLITHIASIS WITHOUT CHOLANGITIS: • Choledocholithiasis is the most common cause of biliary obstruction. • It should be strongly suspected if the jaundice is: • episodic • painful • if ultrasonography has demonstrated the presence of gallstones or bile duct stones.
Workup and Management of Posthepatic Jaundice • SUSPECTED LESION OTHER THAN CHOLEDOCHOLITHIASIS: • clinical presentation is less acute (back pain) • associated constitutional symptoms (e.g., weight loss, fatigue, and long-standing anorexia) • Categories depending on the level of obstruction: • Upper-third obstruction • Middle-third obstruction • Lower-third obstruction
Causes of Posthepatic Jaundice • Upper-third obstruction: • Polycystic liver disease • Caroli disease • Hepatocellular carcinoma • Oriental cholangiohepatitis • Hepatic arterial thrombosis ( after liver transplantation or chemotherapy) • Hemobilia (e.g., after biliary manipulation) • Iatrogenic bile duct injury (e.g., after laparoscopic cholecystectomy) • Cholangiocarcinoma (Klatskin's tumor) • Sclerosingcholangitis • Papillomas of the bile duct
Causes of Posthepatic Jaundice • Middle-third obstruction: • Cholangiocarcinoma • Sclerosingcholangitis • Papillomas of the bile duct • Gallbladder cancer • Choledochal cyst • Intrabiliary parasites • Mirizzi syndrome • Extrinsic nodal compression (e.g., from breast cancer or lymphoma) • Iatrogenic bile duct injury (e.g., after open cholecystectomy) • Cystic fibrosis • Benign idiopathic bile duct stricture
Causes of Posthepatic Jaundice • Lower-third obstruction • Cholangiocarcinoma • Sclerosingcholangitis • Papillomas of the bile duct • Pancreatic tumors • Ampullary tumors • Chronic pancreatitis • Sphincter of Oddi dysfunction • Papillary stenosis • Duodenal diverticula • Penetrating duodenal ulcer • Retroduodenaladenopathy (e.g., lymphoma, carcinoid)
Diagnosis and Assessment of Resectability • The following structures should be carefully evaluated for assessment of the resectability: • superior mesenteric vein • the portal vein • superior mesenteric artery • portahepatis • local adenopathy • extrapancreatic extension • metastasis
Nonoperative Management: Drainage and Cholangiography • Most malignant obstruction present in advance stage and the treatment is usually palliative rather than curative. • Decompression is by ERCP or PTC though the PTC is preferable in obstruction near the bifurcation.
Palliation in patients with advanced malignant disease • supportive care is the only method for treatment of asymptomatic (cholangitis, pruritus ) malignant obstruction. • metalic stent via PTC or ERCP is the option for palliation. • patients who expected to live more than 6 months surgical bypass is preferable. • prophylactic gastric drainage is controversial. • in patients with periampullary tumor, celiac block.
Postoperative Jaundice • Jaundice develops in approximately 1% of all surgical patients after operation. • Common causes of jaundice within 24h after opertation: • Hemolysis as a result of massive blood transfusion, hematoma resorption, or transfusion reaction. • Inhereted disorders of bilirubin metabolism ( Gilbert‘s syndrome and others). • Presence of underlying hemolytic anemia which may exacerbate by administration of drugs.
Summary • Types of jaundice. • Approach to the patient and importance of history and physical examination. • Role of imaging modalities. • Differentiation between surgical and medical jaundice. • Treatment options in surgical jaundice.