Download
1 / 22
571 likes | 2.76k Views
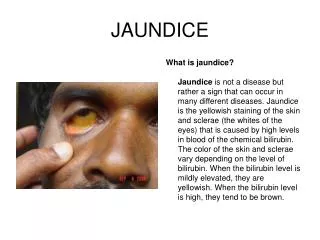
Jaundice. Mohammad Mobasheri SpR General Surgery. Jaundice. Definition: yellow discolouration of skin and sclera as a result of hyperbilirubinaemia Bilirubin >35mmol/L for jaundice to be visible on examination Sclera first place to become jaundiced. Haemoglobin Metabolism.

E N D
Jaundice Mohammad Mobasheri SpR General Surgery
Jaundice • Definition: yellow discolouration of skin and sclera as a result of hyperbilirubinaemia • Bilirubin >35mmol/L for jaundice to be visible on examination • Sclera first place to become jaundiced
Haemoglobin Metabolism • Bilirubin is a product of metabolism of haemoglobin (80%) and other haem containing proteins (e.g. Myoglboin, cytochrome P450: 20%) • Degredation of haemoglobin into bilirubin takes place in macrophages. Bilirubin is then excreted into plasma and binds with albumin RBC breakdown Haemoglobin Haem (iron + porphyrin) Globin Amino Acids Biliverdin Bilirubin (unconjugated) Bilirubin binds to albumin in the plasma
Haemoglobin Metabolism • Uptake of unconjugated bilirubin into hepatocyte • Unconjugated bilirubin converted to conjugated bilirubin by glucuronyl transferase (this is required before bilirubin can be excreted into the bile, as this process makes bilirubin water soluble) • Bilirubin secreted (as component of bile) into the small intestine • Bacterial enzymes deconjugate bilirubin and convert it into urobilinogen • 90% urobilinogen broken down further into stercobilinogen and stercobilin and excreted in faeces • 10% urobilinogen absorbed (via portal vein) • Majority of absorbed urobilinogen re-enters hepatocyte and re-excreted in bile (entero-hepatic circulation) • The rest of the absorbed urolbilinogen bypasses liver and is excreted by kidneys
Hyperbilirubinaemia • Disruption of bilirubin metabolism and excretion can cause hyperbilirubinaemia and subsequent jaundice • Hyperbilirubinaemia maybe unconjugated (indirect) or conjugated (direct) depending on the cause • Some inherited syndromes of bilirubin handling can result in hyperbilirubinaemia • Gilbert’s syndrome – reduced activity of glucuronyl transferase therefore reduced conjugated bilirubin therefore elevated unconjugated bilirubin • Criggler-Najjar – reduction in amount of glucoronyl transferase therefore elevated unconjugated bilirubin • Rotor’s/Dubin-Johnson syndrome – defective excretion of conjugated bilirubin into the biliary cannaliculi therefore elevated conjugated bilirubin
Classification of Jaundice • Pre-hepatic: pathology occuring prior to the liver • Any cause of increased haemolysis (e.g. Spherocytosis, thalassaemia, sickle cell disease, transfusion reaction, auto-immune, malaria etc.) and some drugs • Causes unconjugated hyperbilirubinaemia • Intra-Hepatic: pathology occuring within the liver • All the causes of hepatitis/cirrhosis (e.g. Alcohol, viral, auto-immune, primray biliary cirrhosis, haemochromatosis, wilsons, alpha-1 antitrypsin deficiency etc.), inherited condition on previous slide and some drugs • Can result in hepatocyte destruction and therefore unconjugated hyperbilirubinaemia or in bile cannaliculi destruction and therefore conjugated hyperbilirubinaemia or both • Note/ neonatal jaundice: occurs in most newborns as hepatic machinary for conjugation and excretion of bilirubin not fully matured until 2 weeks of age • Post-hepatic: pathology occuring after conjugation of bilirubin within the liver (aka obstructive jaundice) • Any cause of biliary obstruction (e.g. Gallstones) • Causes conjugated hyperbilirubinaemia
Pre-hepatic/hepatic/post-hepatic? Following investigations will help to determine nature of jaundice: • Liver function tests • Bilirubin • ALT/AST • ALP/GGT • Conjugated v Unconjugated bilirubin levels • Urine bilirubin and urobilinogen levels
Determining aetiology of Jaundice • Total bilirubin and its conjugated and unconjugated levels help to determine nature of jaundice
Determining aetiology of jaundice • Liver Enzymes • ALT/AST mainly present in hepatocytes • ALP/GGT mainly present in bile cannaliculi biliary tree • Derrangement of particular liver enzymes in association with jaundice can determine nature of the jaundice
Determining aetiology of Jaundice • Urine bilirubin • Normally, tiny amount bilirubin (conjugated) excreted in urine • Pre-hepatic jaundice: Haemolysis causes rise in unconjugated bilirubin (water insoluble) and this is not excreted by the kidney therefore there is no rise in urine bilirubin • Some causes of Hepatic jaundice: result in damage to biliary cannaliculi and therefore result in poor biliary drainage and therefore elevated conjugated bilirubin levels in blood, excreted into urine (giving dark urine) • Post-Hepatic juandice: Obstruction to biliary drainage and so conjugated bilirubin (water soluble) levels in the blood increase and appear in the urine (giving dark urine) • Urine urobilinogen • Pre-hepatic jaundice: Haemolysis results in increased bilirubin production and subsequent increase bilirubin metabolism and urobilinogen in stool and therefore in the urine. • Some causes of Hepatic jaundice : result in hepatocellular destruction and therefore reduced re-excretion of re-absorbed urobilinogen (i.e. Reduction in entero-hepatic circulation of urobilinogen) resulting in elevated levels in urine • Post-Hepatic jaundice: Less bilirubin reaching intestine therefore reduction in urobilinogen therefore reduction in urine urobilinogen
Determining Aetiology of Jaundice: History • How long been jaundiced? • Ever been jaundiced before? • Any associated fevers or abdominal pain or weight loss? • Pale stool and dark urine (suggests obstructive/post-hepatic jaundice)? • Any recent foreign travel (hepatitis, malaria)? • Any risk factors for hepatitis (tattoos, IVDU, high risk professions, blood transfusions, multiple sexual partners)? • PMH of blood disorders (e.g. SCD, thalassemia)? • DH any new medications that can cause jaundice? • SH excess alcohol intake • FH of jaundice (inherited disorders of bilirubin metabolism)
Determining aetiology of Jaundice: History • If jaundice associated with background of intermittent RUQ pains think gallstones and choledocholithiasis • If jaundice associated with long history of upper abdominal pain and weight loss and patient elderly thing pancreatic cancer • If jaundice associated with recent foreign travel think hepatitis (A,E) or malaria • If jaundice occuring in patient with risk factors think hepatitis B,C • If jaundice occuring on a background of alcohol abuse think alcoholic liver disease • If jaundice is painless and family history of blood disorder think pre-hepatic jaundice
Investigations • Blood tests • FBC (low HB suggesting haemolysis • LFTs (bilirubin, ALT/AST, ALP/GGT, albumin) • Conjugated and unconjugated bilirubin • Clotting (INR) • U&E (hepatorenal syndrome) • Urine • Bilirubin • Urobilinogen • Above tests used to determine if jaundice pre/intra/post hepatic which will determine further investigations
Investigations • Pre-hepatic • Sickle cell test • Serum electrophoresis • Blood film • Hepatic • Serum iron, ferritin, copper, alpha-1 antitrypsin levels • auto-antibody screen • Hepatitis screen • Liver USS • Post-hepatic • As surgeons we deal with post-hepatic jaundice
Obstructive Jaundice: Causes • Causes • Luminal • Gallstone • Intra-mural • Benign stricture (e.g. As complication of cholecystectomy or due to pancreatitis) • Malignant stricture: cholangiocarcinoma • Extra-mural • Head of pancreas cancer • Pancreatitis (oedema of head of pancreas) • Pancreatic pseudocyst • Compression by malignant lymph nodes at porta hepatis
Obstructive Jaundice: Investigations • Blood tests • FBC (elevated WCC in ascending cholangitis) • U&E (monitor renal function in case of hepato-renal syndrome) • LFTs (elevated bilirubin, ALP/GGT) • Conjugated/unconjugated bilirubin • Clotting (INR maybe elevated) • USS • Look for gallstones, biliary tree dilatation, stone in CBD (though often not seen due to bowel gas). • Look at pancreas to look for cancer (often poor views due to overlying bowel gas) • Look at liver to exclude parenchymal disease.
Obstructive Jaundice: Investigations • CT • Used to assess pancreas in cases of suspected pancreatic cancer • Less sensitive that USS for picking up gallstones • MRCP • Used to assess biliary tree anatomy and determine cause of obstruction (gallstone, stricture) • Diagnostic only but non-invasive • ERCP – performed by gastro-enterologist • Used to assess biliary tree anatomy and determine cause of obstruction • Furthermore, obstruction can be relieved (diagnostic and therepeutic, but invasive) • Stone extraction with balloon trawel • Sphincterotomy • Biliary stent (if stricture: benign or malignant) • Brushings for cytology (if stricture, to look for cholangiocarcinoma)
Obstructive Jaundice: Investigations • PTC (percutaneous transhepatic cholangiogram) – performed by interventional radiologist • Diagnostic and therepeutic (biliary drain to relieve obstruction) but invasive • More invasive and Higher complication rate than ERCP (particularly haemorrhage) therefore used in situations where ERCP unavailable (out of hours in patient with cholangitis) or unsuccesful
Obstructive Juandice: Management • Monitor for acute renal failure (hepato-renal syndrome) • Ensure patients well fluid resuscitated and monitor urine output to reduce the risk of the above • Monitor INR • If derranged give vitamin K • Determine cause of obstructive jaundice • Danger is progression to ascending cholangitis (Charcot’s triad) – can be life threatening! • Must un-obstruct Biliary tree to prevent development of cholangitis
Obstructive Jaundice: biliary decompression • ERCP preferred method • Balloon trawl or dormia basket (for stones) • Sphincterotomy (to prevent future stones from obstructing) • Stent (to allow free drainage of bile past a stricture) • PTC • Used where ERCP unavailable or unsuccesful (as more invasive and higher complication rate) • Drain inserted percuteously, trans-hepatically (through the liver) and into the biliary tree to allow free drainage of bile
Obstructive Jaundice: biliary decompression • Surgical • Most often used in the context of gallstones • At time of cholecystectomy an intra-operative cholangiogram is performed to confirm stones in CBD • If present then consider: • Laparoscopic Trans-cystic (through cystic duct) removal using fogarty catheter • Laparoscopic CBD exploration • In context of malignancy (head of pancreas Ca or external compression by enlarged malignant lymph nodes) • Palliative bypass procedures such as hepaticojejunostomy where ERCP/PTC + stenting has failed
The End Questions?