Download
1 / 25
250 likes | 275 Views
Pathology of Pleura and Mediastinum. Doç. Dr. Işın Doğan Ekici. Pathology of pleura. Pathologic involvement of the pleura is, with rare exceptions, a secondary complication of some underlying pulmonary disease.

E N D
Pathology of Pleura and Mediastinum Doç. Dr. Işın Doğan Ekici
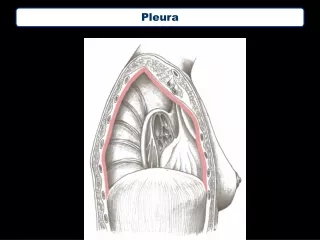
Pathology of pleura • Pathologic involvement of the pleura is, with rare exceptions, a secondary complication of some underlying pulmonary disease. • Secondary infections and pleural adhesions are particularly common findings at autopsy. Important primary disorders include: • (1) primary intrapleural bacterial infections • (2) a primary neoplasm of the pleura known as malignant mesothelioma.
Pleural Effusion and Pleuritis • Pleural effusion, the presence of fluid in the pleural space, can be either a transudate or an exudate. • A pleural effusion that is a transudate is termed hydrothorax. • Hydrothorax from CHF is probably the most common cause of fluid in the pleural cavity. • An exudate, characterized by protein content >2.9gm/dL and, often, inflammatory cells, suggests pleuritis.
The four principal causes of pleural exudate are • (1) microbial invasion through either direct extension of a pulmonary infection or blood-borne seeding (suppurative pleuritis or empyema); • (2) cancer (bronchogenic carcinoma, metastatic neoplasms to the lung or pleural surface, mesothelioma); • (3) pulmonary infarction; and • (4) viral pleuritis.
Other, less common causes of exudative pleural effusions are: • systemic lupus erythematosus, • rheumatoid arthritis, • Uremia, • previous thoracic surgery. • Cancer should be suspected as the underlying cause of an exudative effusion in any patient older than the age of 40, particularly when there is no febrile illness, no pain, and a negative tuberculin test result.
These effusions characteristically are large and frequently are bloody (hemorrhagic pleuritis). • Cytologic examination may reveal malignant and inflammatory cells. • Whatever the cause, transudates and serous exudates are usually resorbed without residual effects if the inciting cause is controlled or remits. • In contrast, fibrinous, hemorrhagic, and suppurative exudates may lead to fibrous organization, yielding adhesions or fibrous pleural thickening, and sometimes minimal to massive calcifications.
Pneumothorax • Pneumothorax refers to air or other gas in the pleural sac. • It may occur in young, apparently healthy adults, usually men without any known pulmonary disease (simple or spontaneous pneumothorax), or as a result of some thoracic or lung disorder (secondary pneumothorax), such as emphysema or a fractured rib. • Secondary pneumothorax occurs with rupture of any pulmonary lesion situated close to the pleural surface that allows inspired air to gain access to the pleural cavity. • Such pulmonary lesions include emphysema, lung abscess, tuberculosis, carcinoma, and many other, less common, processes. • Mechanical ventilatory support with high pressure may also trigger secondary pneumothorax.
Complications of pneumothorax • There are several possible complications of pneumothorax. • A ball-valve leak may create a tension pneumothorax that shifts the mediastinum. • Compromise of the pulmonary circulation may follow and may even be fatal. If the leak seals and the lung is not re-expanded within a few weeks (either spontaneously or through medical or surgical intervention), so much scarring may occur that it can never be fully re-expanded. • In these cases, serous fluid collects in the pleural cavity and creates hydropneumothorax. • With prolonged collapse, the lung becomes vulnerable to infection, as does the pleural cavity when communication between it and the lung persists. • Empyema is thus an important complication of pneumothorax (pyopneumothorax). • Secondary pneumothorax tends to be recurrent if the predisposing condition remains. What is less well recognized is that simple pneumothorax is also recurrent.
Hemothorax & Chylothorax • Hemothorax, the collection of whole blood (in contrast to bloody effusion) in the pleural cavity, is a complication of a ruptured intrathoracic aortic aneurysm that is almost always fatal. • With hemothorax, in contrast to bloody pleural effusions, the blood clots within the pleural cavity. • Chylothorax is a pleural collection of a milky lymphatic fluid containing microglobules of lipid. The total volume of fluid may not be large, but chylothorax is always significant because it implies obstruction of the major lymph ducts, usually by an intrathoracic cancer (e.g., a primary or secondary mediastinal neoplasm, such as a lymphoma).
Malignant mesothelioma • Malignant mesothelioma is a rare cancer of mesothelial cells, usually arising in the parietal or visceral pleura, although it also occurs, much less commonly, in the peritoneum and pericardium. It has assumed great importance because it is related to occupational exposure to asbestos in the air. • Approximately 50% of individuals with this cancer have a history of exposure to asbestos. • Those who work directly with asbestos (shipyard workers, miners, insulators) are at greatest risk, but malignant mesotheliomas have appeared in persons whose only exposure was living in proximity to an asbestos factory or being a relative of an asbestos worker.
The latent period for developing malignant mesotheliomas is long, often 25 to 40 years after initial asbestos exposure, suggesting that multiple somatic genetic events are required for tumorigenic conversion of a mesothelial cell. • The combination of cigarette smoking and asbestos exposure greatly increases the risk of bronchogenic carcinoma, but it does not increase the risk of developing malignant mesotheliomas.
Morphology • Malignant mesotheliomas are often preceded by extensive pleural fibrosis and plaque formation, readily seen in computed tomographic scans. • These tumors begin in a localized area and in the course of time spread widely, either by contiguous growth or by diffusely seeding the pleural surfaces. • At autopsy, the affected lung is typically ensheathed by a yellow-white, firm, sometimes gelatinous layer of tumor that obliterates the pleural space. • Distant metastases are rare. • The neoplasm may directly invade the thoracic wall or the subpleural lung tissue. Normal mesothelial cells are biphasic, giving rise to pleural lining cells as well as the underlying fibrous tissue.
Histologically, mesotheliomas conform to one of three patterns: • (1) epithelial, in which cuboidal cells line tubular and microcystic spaces, into which small papillary buds project; this is the most common pattern and also the one most likely to be confused with a pulmonary adenocarcinoma; • (2) sarcomatoid, in which spindled and sometimes fibroblastic-appearing cells grow in nondistinctive sheets; and • (3) biphasic, having both sarcomatoid and epithelioid areas.
Asbestosis and carcinogenesis • The basis for the carcinogenicity of asbestos is still a mystery. Asbestos is not removed or metabolized from the lung, and hence the fibers remain in the body for life. • Thus, there is a lifetime risk after exposure that does not diminish with time (unlike smoking, in which the risk decreases after cessation). • It has been hypothesized that asbestos fibers preferentially gather near the mesothelial cell layer, where they generate reactive oxygen species that cause DNA damage and potentially oncogenic mutations. Somatic mutations of two tumor suppressor genes (p16/CDKN2A on chromosome 9p21 and NF2 on chromosome 22q12) have been observed in malignant mesotheliomas. • Recent work has demonstrated the presence of simian virus 40 viral DNA sequences in 60% to 80% of pleural malignant mesotheliomas and in a smaller fraction of peritoneal cases. • The simian virus 40 T-antigen is a potent carcinogen that binds to and inactivates several essential regulators of growth, such as p53 and RB. Not everyone is convinced that this association is causal and currently, the interaction of asbestos and simian virus 40 in mesothelioma pathogenesis is an area of active investigation.
Pathology of mediastinum • Mediastinum is thoracic cavity between pleural cavities, from sternum to spine, thoracic inlet to diaphragm. Major tumors or lesions of mediastinum are: • Superior mediastinum: thymomas, thymic cyst, lymphoma, thyroid lesions, parathyroid adenoma • Anterior mediastinum: ventral to anterior cardiac border and aortic root - thymic epithelial tumors and cysts, germ cell neoplasms, lymphoproliferative lesions, retrosternal thyroid glandular proliferations, parathyroid lesions, aorticopulmonary-type paragangliomas, lymphangioma, hemangioma, lipoma • Middle mediastinum: between (a) anterior cardiac silhouette and aortic root and (b) posterior tracheal carinii - pericardial cyst, bronchogenic cyst, lymphoma • Posterior mediastinum: dorsal to large conducting airways - neurogenic tumors: schwannoma, neurofibroma, ganglioneuroma, ganglioneuroblastoma, MPNST, neuroblastoma, paraganglioma, gastroenteric cysts.
Inflammatory disorders of mediastinum • Acute mediastinitis • Chronic mediastinitis • Sclerosing mediastinitis
Acute mediastinitis • Usually in posterior mediastinum, due to traumatic perforation of esophagus or descending infection along prevertebral fascia • Initial lesion may be a neck abscess • Often causes mediastinal abscess which requires surgical drainage • Other causes: chest wall infection or post-cardiac surgery, often due to CMV
Chronic mediastinitis • May compress superior vena cava and simulate malignancy • Usually anterior to tracheal bifurcation • Some cases may represent fibrosing mediastinitis
Sclerosing mediastinitis • Also called idiopathic mediastinal fibrosis • A fibroinflammatory lesion of mediastinum associated with other idiopathic fibrosing conditions such as retroperitoneal fibrosis, sclerosing cholangitis, Riedel’s struma, inflammatory pseudotumor of orbit • Also associated with pulmonary or mediastinal nodal infection due to Histoplasma or other fungi; trauma, syphilis, methysergide treatment, phlebitis • Usually anterosuperior mediastinum, presenting at any age, often with superior vena cava syndrome or cardiorespiratory compromise • Xray: asymmetric mediastinal widening with projection of mass into upper lung field • Treatment: steroids, surgical excision • Gross: dense white fibrosis, well demarcated from surrounding tissue • Micro: different patterns - cellular fibrous reaction with polymorphic inflammatory infiltrate with plasma cells and eosinophils; dense, fibrohyaline tissue with focal spindle cells and inflammatory cells or scattered lymphoid follicles with occasional dystrophic calcification could be seen.
Cystic lesions of mediastinum: • 10-15% of radiologically detected mediastinal masses • Often developmental cysts: • Thymic, pericardial, bronchogenic, enteric, parathyroid cysts or mixtures could be seen