Download
1 / 20
200 likes | 282 Views
DCH GUIDELINES FOR CHILDHOOD UTI (Informed by NICE). ROLLO CLIFFORD 2008. PURPOSE. Consitent strategy for: Management Investigation Future prevention Further follow up. DCH.

E N D
DCH GUIDELINES FOR CHILDHOOD UTI(Informed by NICE) ROLLO CLIFFORD 2008
PURPOSE • Consitent strategy for: • Management • Investigation • Future prevention • Further follow up
DCH • aims to select out children for detailed investigation and follow up whilst causing the least disruption to the lives of those at lowest risk.
Suspecting UTI in Infants • Reduced feeding or Vomits more than usual. • Fever with no other obvious explanation. • Sleepy and lethargic • Stops gaining weight or unexpected loss. • Has jaundice which gets worse when more than a week old. • (Unusual smell to urine) • (Seems to be in pain at times and when urine is passed)
Urine Collection ProtocolMessages for Primary Care • MSU, CCU, Pad OK – Bag not. • Stick test can exclude if negative to both nitrites and leucocytes. • But send to lab anyway and consider treatment if: • Under 3 years • Symptoms highly suggestive. • If positive to either send + consider treat.
Treatment • Treat rapidly if upper tract features • Infants nearly always in this category • Urine sample essential – Murphy’s law! • Amoxycillin excellent – if sensitive – toss a coin? • Trimethoprim/Augmentin/Cephalexin • Hospital if unable to take or ill
The History - PC, PMH, FH • Initial symptomatology – fever, vomiting, site of pain/discomfort • Method of urine collection • Previous infections • Family history - renal problems and hypertension
Poos and Wees • Dysfunctional Elimination Syndrome • Urge syndrome • Staccato voiding • Fractional and incomplete voiding • Voiding postponement • Constipation Constipation and DES are both strongly associated with recurrent UTI and Reflux
The History - voiding and bowels Symptoms between episodes – recurrent loin pain, enuresis, encopresis, neurological symptoms affecting lower limbs Bowel habit - constipation, dietary history. Potty training Voiding pattern – staccato voiding, postponement, vaginal reflux (legs held together during micturition) Other voiding issues – footstool for younger children, school toilets..
The History – other risks • Fluid intake – too few drinks or, in some cases, interfering with appetite. • Hygiene – bubble baths, washing hair in bath, frequency, wiping, odour. • Symptoms suggestive of thread work infection.
Examination • Plotted height and weight with comparison with previous centiles • Blood pressure measurement • Abdominal examination • Genital examination in pre-pubertal children (unless recorded normal elsewhere) • Urinalysis
Ultrasound • Renal size • Dilation of collecting system and ureter • Bladder emptying • Congenital abnormality • Large calculi • No – ionising radiation • Atraumatic • Costs about 1/10 of an isotope scan
Advice and prevention • Symptoms of infection (infants especially) • Prevention of future infection • Provide leaflet • Treat constipation – dietary advice / lifestyle / laxatives in some
Ultrasound • Hopeless at picking up scarring but: • May find abnormality associated with scarring.
Ultrasound • NICE – limited to: • Infants • Children with atypical or recurrent infections • Halves number of ultrasounds but may miss 2/3 of significant abnormalities. • Local protocol – continue with USS for all children. • Prospective audit?
Ultrasound can: • Assess renal size • Collecting system or ureteric dilatation • Evaluate the bladder (including emptying). • Can indicate obstruction and other congenital abnormalities of the urinary tract’ • Can detect large calculi • No ionising radiation and is non-invasive • Cost – 1/10th cost of DMSA
Ultrasound can not: • Exclude scarring • Exclude reflux – which may predispose to future scarring.
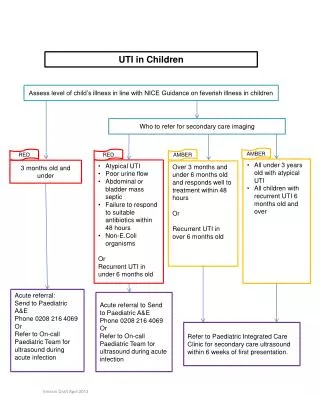
Referral 1° to 2 ° - acute • Severe systemic upset • Inadequate fluid intake/vomiting • Infants
Referral 1 ° to 2° - Letter • Any upper tract symptoms – fever >38, loin pain, vomiting, obvious systemic upset. • Two or more infections • Any abnormality on ultrasound. • Diagnostic doubt • Associated risk factors which prove difficult to manage – e.g. constipation/soiling. • GP preference
Referral 1 ° to 2° - Telephone • Symptoms or ultrasound findings suggest severe obstruction (e.g. Possible urethral valves / gross renal or ureteric dilation on ultrasound – particularly if during infancy and if bilateral)