Download
1 / 22
220 likes | 390 Views
DCH GUIDELINES FOR CHILDHOOD UTI (Informed by NICE). ROLLO CLIFFORD. UTI in 30mins. Diagnosis Treatment Assessment: History Examination Referral. DIAGNOSIS. Suspecting UTI in Infants. Reduced feeding or Vomits more than usual. Fever with no other obvious explanation.

E N D
DCH GUIDELINES FOR CHILDHOOD UTI(Informed by NICE) ROLLO CLIFFORD
UTI in 30mins • Diagnosis • Treatment • Assessment: • History • Examination • Referral
Suspecting UTI in Infants • Reduced feeding or Vomits more than usual. • Fever with no other obvious explanation. • Sleepy and lethargic • Stops gaining weight or unexpected loss. • Has jaundice which gets worse when more than a week old. • (Unusual smell to urine) • (Seems to be in pain at times and when urine is passed)
Urine sample essential – if do not, Murphy’s law tends to apply!
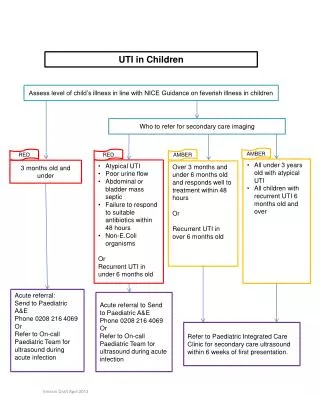
Urine Collection ProtocolMessages for Primary Care • MSU, CCU, OK – Bag not. • Stick test – if positive to nitrites or leucocytes, lab sample + consider Rx. • Lab sample as urgent if: • Known urinary tract anomaly • Symptoms suggestive of pyelonephritis • Under 3 years with suggestive symptoms • White cap bottle if small sample but to labe quickly.
Key Messages • Treat rapidly if upper tract features • Infants nearly always in this category • Amoxycillinexcellent – if sensitive – toss a coin? • Trimethoprim/Augmentin/Cephalexin • Follow up and check sensitivities
Presentation • Initial symptomatology • Fever • Vomiting • Site of any pain/discomfort • Diagnostic accuracy – method of urine collection
PMH / FH • Previous infections / undiagnosed fevers • Recurrent loin pain • Possible neurological symptoms • Family history – renal anomalies, renal failure, hypertension
Poosand Wees • Dysfunctional Elimination Syndrome • Urge syndrome • Staccato voiding • Fractional and incomplete voiding • Voiding postponement • Constipation / Stool retention / Enuresis Soiling • Vaginal reflux
Other Issues and Risks • Fluid intake – too few drinks or, in some cases, interfering with appetite. • Hygiene – bubble baths, washing hair in bath, frequency, wiping, odour. • Symptoms suggestive of thread worm infection. • School toilets and access
Examination • Plotted height and weight with comparison with previous centiles • Blood pressure measurement • Abdominal examination • Genital examination in pre-pubertal children (unless recorded normal elsewhere) • Urinalysis
Investigation - ultrasound For all under 4 or in referral categories • Renal size • Dilation of collecting system and ureter • Bladder emptying • Congenital abnormality • Large calculi • No – ionising radiation • Atraumatic • Costs about 1/10 of an isotope scan
Ultrasound can not: • Exclude scarring • Exclude reflux – which may predispose to future scarring.
Who does not need referral? • Symptoms of cystitis only – i.e. No upper tract symptoms • Age >12 months • Clear diagnosis • Normal ultrasound • Single infection • Associated factors e.g. Constipation/soiling, manageable in primary care • Time to make above assessment with confidence.
Advice and prevention • Recogntion of infection (infants especially) • Prevention of future infection • Bladder habit • Hygiene issues • Diet (incl. fluids) and Constipation • Provide leaflet
Acute Referral • Severe systemic upset • Inadequate fluid intake/vomiting • Infants
OP Referral • Any upper tract symptoms – fever >38, loin pain, vomiting, obvious systemic upset. • Two or more infections • Any abnormality on ultrasound. • Diagnostic doubt • Associated risk factors which prove difficult to manage – e.g. constipation/soiling. • GP preference
Urgent discussion - telephone • Symptoms or ultrasound findings suggest severe obstruction (e.g. Possible urethral valves / gross renal or ureteric dilation on ultrasound – particularly if during infancy and if bilateral)