Download

1 / 98
980 likes | 1.18k Views
Endocrine system. medications. HORMONES. Active chemical substances secreted into bloodstream from endocrine glands Initiate or regulate activity of an organ or group of cells. HORMONES. Physiological effects: Metabolism Growth Homeostasis Integration . HORMONES. Hypothalamic factors

E N D
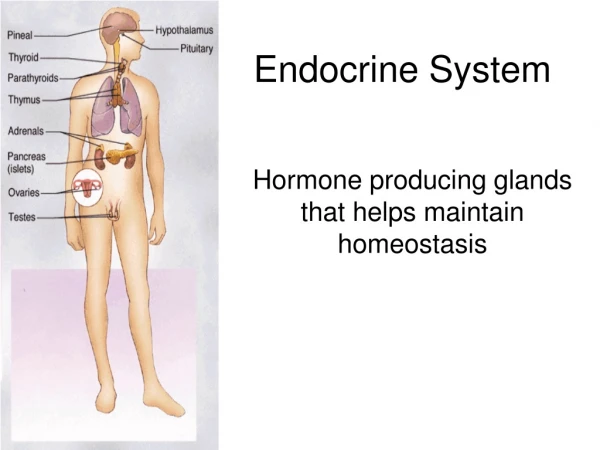
Endocrine system medications
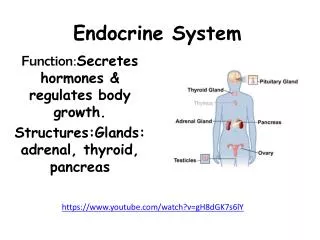
HORMONES Active chemical substances secreted into bloodstream from endocrine glands Initiate or regulate activity of an organ or group of cells
HORMONES • Physiological effects: • Metabolism • Growth • Homeostasis • Integration
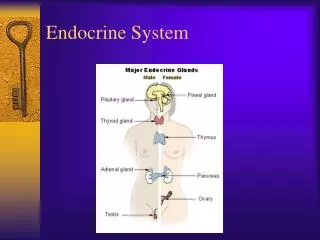
HORMONES • Hypothalamic factors • Anterior and posterior pituitary gland hormones • Thyroid hormones • Parathyroid hormones • Pancreatic insulin and glucagon
HORMONES • Steroid hormones from the adrenal cortex • Gonadal hormones
HORMONES • Major development of the 20th century • Identified the chemical structure of most hormones • Now able to synthesise and replicate
ENDOCRINE GLANDS • Groups of cells that produce and secrete hormones • Transported in the blood typically bound to proteins • Only free hormones are available to act at receptors or to cross membranes
HORMONES • The chemical class of a hormone • Steroid • Amino-acid derived • Polypeptides • Simple proteins
HORMONES • Clinical significance of chemical class is that it affects how the hormone can be administered • Peptide and protein hormones cannot be given orally
GENERAL FUNCTIONS OF HORMONES • Regulate secretions and motor activity of the GIT • Energy production • Composition and volume of extracellular fluid • Adaptation and immunity
GENERAL FUNCTIONS OF HORMONES • Growth and development • Reproduction and lactation
Endocrine disorders • Disorders usually involve either over production or underproduction of hormones • Treatment may involve surgery, anti hormones or replacement hormone therapy
DIABETES MELLITUS MEDICATIONS ADMINISTRATION
DIABETES MELLITUS • A metabolic disorder causing disturbance of body’s capacity to utilize • Sugar • Fat • Protein
DIABETES MELLITUS • Due to: • Insulin deficiency • Insulin resistance
DIABETES MELLITUS • Result; • Elevated blood glucose • Body unable to utilize glucose without insulin • Body draws on fat and protein to supply fuel for energy • Carbohydrate necessary to complete fat embolism
DIABETES MELLITUS • Result; • Ketones accumulate in blood • Protein breakdown leads to; • Weight loss • Weakness • Hyperglycaemia • Lethargy
DIABETES MELLITUS • Types of diabetes • Type 1 insulin dependant diabetes • IDDM • Type 2 non-insulin dependant diabetes • NIDDM • Secondary diabetes • Gestational diabetes • Mature onset diabetes of the young
DIABETES MELLITUS • Diabetes affects 0.5% to 4% of the population depending on; • Type of diabetes • Age group • Ethnic group • Incidence appears to be increasing in older age group
DIABETES MELLITUS • Insulin dependant diabetes mellitus; IDDM; Type 1 diabetes. • Usually affects • Children • Young adults
DIABETES MELLITUS • Symptoms develop over short space of time (2 – 3 weeks) • An auto-immune disease • Beta cells of the pancreas are destroyed • Urine glucose levels increased • Ketones will be developed in urine • Patient may present with keto-acidosis
DIABETES MELLITUS • Classic symptoms; • Polydipsia • Polyuria • Lethargy • Weight loss • Infected wounds which will not heal • Pruritis
DIABETES MELLITUS • Types of diabetes; • Type 2 diabetes, non-insulin diabetes NIDDM • May present with established complication • Neuropathy • Cardiovascular disease • Retinopathy • Classic symptoms • Less obvious • Appear over a longer period of time • Treatment reduces symptoms
DIABETES MELLITUS • NIDDM • Risk group • Obese • Over 40 years of age • Closely related to people with diabetes • Women who have large babies • Women who have had gestational diabetes
DIABETES MELLITUS • Pancreas • lies transversely across abdomen • Secretes about 1200 – 1500 mls of clear fluid per day containing water, sodium bicarbonate, salts & digestive enzymes that digest proteins, fats, carbohydrates & nucleic acids • These are exocrine functions of the gland
DIABETES MELLITUS • Between exocrine cells are small pockets of endocrine tissue known as pancreatic islets or Islets of Langerhanswhich make up 2% of the weight of the pancreas • These cells produce hormones which are secreted into the blood stream and are involved in nutrient balance, particularly blood sugar levels, & gastrointestinal (GI) functions
DIABETES MELLITUS • Pancreas: • Different cells produce different hormones • Insulin produced by beta cells • Glucagon produces by alpha (A) cells • Somatostatin (GHRIF) by delta (D) cells • Somatostatin has significant effects not only to inhibit release of growth hormone, but also to inhibit release of insulin & glucagon (see Bryant et al chapter 38, p 61 for further information about somatostatin
DIABETES MELLITUS • Aetiology of diabetes mellitus • Increased levels of blood glucose • Decreased entry of glucose to the cells • Impairment of cellular ability to use glucose • Free fatty acids released from fatty tissue to provide energy source for tissues • Oxidation of fatty acids in liver produce ketone bodies
DIABETES MELLITUS • Aetiology of diabetes mellitus (cont) • If the production of these substances is faster than the the body is able to metabolise them the pH of body fluid falls = acidosis • Acidosis can lead to altered respiration, nervous system depression, coma & death • Protein synthesis decreases
DIABETES MELLITUS • Aetiology of diabetes mellitus (cont) • Protein breakdown increases • Leads to weight loss, increased susceptibility to infection, poor tissue repair • Appearance of glucose and ketone bodies in the urine • Glycosuria upsets osmotic balance & extra water is required to excrete glucose and ketones leading to polyuria
DIABETES MELLITUS • Aetiology of diabetes mellitus (cont) • Polyuria leads to • Strong sense of thirst • Polydipsia • Dehydration may occur • Circulatory problems such as hypotension may present
DIABETES MELLITUS • Aetiology of diabetes mellitus (cont) • Long term complications due to high glucose levels include damage to blood vessels and nerves causing • Renal insufficiency • Retinal damage • Atherosclerosis • Coronary artery disease is most common cause of death
DIABETES MELLITUS • Management is achieved by monitoring of • Blood glucose levels • Dietary control • Exercise routine • Monitoring and management of infections, weight and exercise and rest patterns
DIABETES MELLITUS • Blood glucose management of IDDM • Ideal testing times ½ hour before meals and at night (may be 3-5 times per day) • Insulin injections which are direct replacement for the insulin which would normally be produced by the pancreas • Artificial delivery of insulin by sub-cutaneous injection at prescribed times depending on type of insulin used
DIABETES MELLITUS • NIDDM medications • Two main types of medication • SULPHONYLUREAS • These drugs stimulate the pancreas to produce insulin • BIGUANIDES • These drugs reduce the absorption of glucose from the gut and also promote weight loss
DIABETES MELLITUS • INSULIN • Body’s main fuel storage hormone • Secreted by pancreatic beta cells in response to increased levels of glucose in the body • Overall function is to ensure that tissues have sufficient chemical substrates for energy, storage, anabolism & repair
DIABETES MELLITUS • INSULIN • Insulin is released into the portal system • Most important stimulus is raised blood sugar levels • Insulin release is inhibited by somatostatin & adrenaline
DIABETES MELLITUS • INSULIN (cont) • Deficiencies of release occur in: • Pancreatic disorders • Diabetes mellitus • Pancreatitis • Other endocrine disorders • Cushings disease • Acromegally
DIABETES MELLITUS • INSULIN (cont) • Deficiencies of release can be caused by drugs • See table Bryant et al p 640 Table 41-2 for drugs which may cause hyperglycaemia and hypoglycaemia • Exercise: • Choose two drugs from each category & using your books & working in pairs, discuss the action of these drugs and your nursing actions in management of patients who may display the response to either the hypoglycaemis or hyoerglycaemic effects. Document your findings
DIABETES MELLITUS • INSULINS • Ultra short acting - onset 15 minutes • Peak effect 1 hour / duration of action 4-5 hrs • Short acting- onset 30 minutes • Peak effect 2-5 hrs / duration of action 6-8 hrs • Intermediate acting – 1 - 2.5 hours • Peak effect 4-12 hrs / duration 6-24 hrs
DIABETES MELLITUS • Long acting 2-6 hours • Peak effect 10-20hrs / duration 24-26hrs • Combinations 0.5-1 hour • Peak effect 1-12 hrs / duration 16-18 hrs • Long acting 24 hours • Glargine (Lantus) potentially more suitable than NPH insulin Shown to decrease HbA1C and the frequency of hypoglycaemia
DIABETES MELLITUS • NURSING MANAGEMENT • Important to ensure that blood glucose readings are • Accurate • Documented accurately • Checked if reading is outside of the normal range for the patient • Reported & recorded
INSULIN ADMINISTRATION • Choose correct syringe size • Check dose of insulin (s) to be administered • Follow drug administration protocols • Draw up correct dose of insulin • Administer to patient in appropriate site
INSULIN ADMINISTRATION • Insulin syringes • 30 units • 50 units • 100 units
INSULIN ADMINISTRATION • Types of insulin • Rapid acting • Short acting • Intermediate acting • Premixed insulin • Premixed insulin Lispro • Refer to accompanying chart from Lilly
INSULIN ADMINISTRATION • Mixing insulins • Clear - regular • Cloudy - isophane • Withdraw amount of clear from clear vial • Keep control of plunger and withdraw amount of cloudy from cloudy vial • If you make a mistake discard and start again • Always draw clear insulin up first
INSULIN ADMINISTRATION • Prepare patient • Administer dose • Unless there are facility protocol reasons it is not necessary to swab skin before or after administration • Do not rub site after administration • You may press firmly on skin with a dry swab if fluid appears on skin
INSULIN ADMINISTRATION • Insulin injections given by • Insulin syringes • Insulin pens • Insulin pumps
INSULIN ADMINISTRATION • Syringes are set to deliver the amount of insulin in units as is stated on the syringe • Insulin pens deliver premixed or single types of insulin through a pen with a dial up amount • Insulin pumps are attached to the patient via a fine needle and tubing and are programmed to the client’s needs
INSULIN ADMINISTRATION • Mixing insulin in a single syringe • Insulin comes in a variety of time of action in the body • The clear insulin is short acting • The cloudy insulin will be slower acting and have different lengths of time for insulin delivery to the client