Download
1 / 40
420 likes | 603 Views
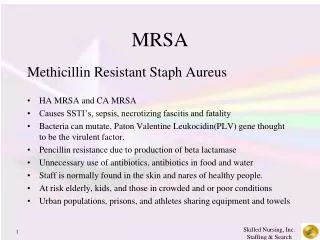
MRSA. Phillip O. Coffin, MD MIA Division of Infectious Disease, CPMC Director of Substance Use Research, SFDPH Assistant Clinical Professor, UCSF. Disclosures. Sadly, none. Outline. Definition When / how to treat Cases. ccr. mec A. Antibiotic resistance genes. mec A. ccr.

E N D
MRSA Phillip O. Coffin, MD MIA Division of Infectious Disease, CPMC Director of Substance Use Research, SFDPH Assistant Clinical Professor, UCSF
Disclosures Sadly, none
Outline • Definition • When / how to treat • Cases
ccr mecA Antibiotic resistance genes mecA ccr CA-MRSA is genetically distinct from HA-MRSA • Novel SCC mec element (type IV) • Lack of multiple antibiotic resistance genes • Presence of additional genetic elements, potential virulence factors (Panton-Valentine leukocidin, ACME, phenol-soluble modulins etc.) CA-MRSA Type IV HA-MRSA Type I-III
Epidemiology of MRSA Infection in San Francisco USA300 Miller and Diep Clinical Infectious Diseases 2008
Who “has” MRSA (or SA)? Infection image
Antibiotic options Outpatient • Trim-sulfa (2 tabs DS BID) • Doxycycline • Linezolid • Clindamycin Inpatient • Vancomycin • Linezolid (ZyvoxTM) • Daptomycin (CubicinTM) • Telavancin(VibativTM) • Ceftaroline (TeflaroTM) • Tigecycline (TygacilTM) • Quinupristin/dalfopristin
Additives • Rifampin • Gentamicin • Beta-lactams
Linezolid • Pros • May treat other foci (bone, lung) poorly penetrated by other drugs • 100% oral bioavailability • Case reports suggest efficacy in R-sided endocarditis • Cons • Toxicity profile • Bacteriostatic • Limited data • Typically used in combo with cidal drug • Relapse
Daptomcyin • Pros • Convenient dosing • Not nephrotoxic • Bactericidal • Potent in animal models • Most evidence based • Cons • FDA approved dose too low • Resistance emerges on therapy • Toxicity at higher doses? • Cross-resistance with VISA
Telavancin • Pros • Bactericidal • Potent in animal models • Active against VISA • Once daily dosing • Cons • Nephrotoxic • Only 3 (very messy) cases • May have cross-sensitivity with vancomycin
Ceftaroline • Pros • Bactericidal • Potent in animal models • Active against VISA • Beta-lactam safety profile • Cons • Uncertain dosing • Limited clinical experience, only 16 cases
Mortality: Linezolid v. Vancomycinfor MRSA HAP/VAP Wunderink, et al, Clin Infect Dis 54:621, 2012 Mark Kunkel: Abstract 5047, IDSA 2010 Annual Meeting
Decolonization • Administration of topical antimicrobial or antiseptic agents, with or without systemic antimicrobial therapy, to colonized patients for the purposes of eradicating or suppressing the carrier state. • Prevent transmission to others, thereby preventing infection in other patients • Prevent endogenous infection
Decolonization: PRO • 2008 Cochrane Review: Mupirocin for prevention of S. aureus infections in nasal carriers • 9 RCTs: 4 surgical; 3 dialysis; 1 non-surgical; 1 MRSA colonized • in rate of nosocomial S. aureus infection • All studies (RR 0.55, 95% CI 0.34-0.89) • High-quality studies (RR 0.69, 95% CI 0.47-1.00) • Benefit in surgical, dialysis pts; none in non-surgical pts, MRSA carriers • No in rate of S. aureus surgical site infections • RR 0.63, 95% CI 0.38-1.04 Van Rijen Cochrane Reviews 2008
Decolonization: CON • 2003 Cochrane Review: Antimicrobial drugs for treatment of MRSA colonization • 6 RCTs: all prior to CA-MRSA, variety of topical and systemic therapies • No in MRSA carriage rates • One study, short-term eradication at 30, not 90 days • Adverse events with systemic agents, emergence of resistance • Recolonization occurs in about 25% of successful cases within 4 weeks; 50-75% after a few months Van Rijen Cochrane Reviews 2008
Regimens • Topical • Nasal mupirocin 2% bid x5-7 days • chlorhexidine 2-4% baths daily • +/- trim-sulfa or doxycycline • +/- environmental / family decontamination 1Van Rijen Cochrane Reviews 2008
32 y/o man with 3 days of an enlarging, painful lesion below his L knee which he attributes to a “spider bite”. T 37.3 BP 118/70 P 82 Case 1
What is the appropriate management? • Incision and drainage alone • Incision and drainage plus oral anti-MRSA antimicrobial agent • Oral anti-MRSA antimicrobial agent
Management of Abscess Primary Rx - incision & drainage (AII) No difference in outcomes whether an active antibiotic is used1 Randomized trial of patients with skin abscesses (mostly MRSA), high cure rates in all: cephalexin (84.1%); placebo (90.5%)2 Additional benefit of MRSA active oral antibiotic beyond I&D is unknown; clinical trials underway. Consider empiric Rx for CA-MRSA if: systemic symptoms, severe local symptoms, immunosuppression, extremes of patient age, critical location, failure to respond to I&D 1Lee MC PIDJ ‘04; Young DM Arch Surg‘04; Fridkin SK NEJM ‘05; Moran G NEJM ‘06 2Rajendran PM AAC’07
42 year old F presents w/ progressive erythema of her L lower leg x 24 hours. T 37.0 BP 132/70 P 78 Case 2
What is the appropriate management? • Clindamycin 300 mg PO tid • Amoxicillin 875 mg PO bid, monitor clinically with addition of TMP/SMX if no response • Amoxicillin 875 mg PO bid and TMP/ SMX 2 DS tab PO bid
Management of Uncomplicated Cellulitis With purulent drainage: Empiric Rx for CA-MRSA is recommended (AII). Pure cellulitis*: Empiric Rx for -hemolytic streptococci is recommended. Empiric Rx for CA-MRSA may be considered (CIII). (Moran GJ NEJM 2006) *Pure cellulitis: without purulent drainage, focal induration, associated abscess
Uncomplicated SSTIs: Antimicrobial Therapy Empiric oral antimicrobial therapy for CA-MRSA: Clindamycin, trimethoprim-sulfamethoxazole (TMP/SMX), or a tetracycline* (e.g. doxycycline or minocycline) (AII) If empiric therapy for -hemolytic streptococci and CA-MRSA is clinically indicated: Clindamycin (AIII) OR -lactam (e.g. amoxicillin) and TMP/SMX or a tetracycline* (AIII) NIH-sponsored clinical trials underway *Avoid in children < 8 years old
Management of Complicated SSTIs Management of cSSTI and necrotizing fasciitis Surgical evaluation and debridement (AIII) Empiric Rx for MRSA is recommended1(AII) Empiric Rx for MRSA cSSTI and necrotizing fasciitis Vancomycin, daptomycin2, linezolid3, tigecycline4(AI) No significant difference in primary outcome of clinical cure 1Kollef MH CID 2008; Miller LG NEJM 2005; Young LM Surgical Infections 2008. 2Arbeit RD et al CID 2004; 3Weigelt J et al AAC 2005; 4Breedt J AAC 2005
35 y/o man presents with 4 days of fever, chills, myalgias, and cough. Now with increasing dyspnea and hemoptysis x 24 hours. T38.7 P120 BP96/60 R28 92%RA Moderate respiratory distress with coarse rhonchi 15>44<425, left shift Rapid flu: + influenza A Case 3 Frazee B. Ann Emerg Med. 2006
In addition to starting anti-influenza therapy, would you treat with antibiotics and if so which? • None • Ceftriaxone and azithromycin • Vancomycinandcefepime • Vancomycinand ceftriaxone and azithromycin • Linezolid andcefepime
Is MRSA a cause of community-acquired pneumonia (CAP)? • MRSA is an infrequent cause of CAP, empiric Rx for MRSA not routinely recommended1 • MRSA: a complication of influenza? • 2003-04 and 2006-07 influenza seasons2 • majority of staphylococcal CAP was due to MRSA • morbidity & mortality • No clinical, laboratory, radiographic findings that distinguish patients with MRSA from other etiologies of CAP 1IDSA/ ATS 2007 CAP guidelines; 2Hageman JC EID 2006; Kallen A Ann Emerg Med 2008
Management of MRSA Pneumonia Empiric Rx for MRSA is recommended for patients with severe CAP and1…(AIII) Preceding/concurrent influenza-like illness Necrotizing or cavitary infiltrates ICU admission Vancomycin or linezolid is recommended(AII). Superiority of either antibiotic unclear2 Daptomycin is not indicated in PNA 1Francis JL CID 2005; Gonzalez BE Clin Infect Dis 2005; Hageman JC EID 2006; MMWR 2007; Mandell L CID 2007; Finelli L Pediatrics 2008; 2Rubinstein E CID 2001; Wunderink RG Clin Therap 2003; Wunderink RG Chest 2003;
Case 4 • 45 y/o man w/ 5 days of an enlarging, painful buttock lesion now with 2 days of fever/chills • T 38.5 BP 103/67 P 104 RR 16 Wt: 100 kg • Obese • Heart: 2/6 systolic murmur at RUSB • Right buttock: 6 x 2 cm tender, fluctuant mass with purulent drainage and surrounding erythema
Case 4 (continued) • Labs: 12.5 > 38 > 350; Cr 0.8 • Started on Vancomycin 1g IV q12 hrs • HD #1 blood cx: 2/2 MRSA • HD #3 blood cx: 2/2 MRSA • TTE: 5 mm vegetation on tricuspid valve • Vancomycin trough: 9.2 g/mL
In addition to I&D, what is the most appropriate management of this patient? • Add gentamicin to vancomycin • Add rifampin to vancomycin • Increase vancomycin dose to 1.5 g IV q12, and adjust to achieve goal trough of 15-20 g/mL • Discontinue vancomycin and start IV daptomycin
Median duration of S. aureus bacteremia • MRSA: 7-9 days • MSSA: 3-4 days Levine Ann Intern Med 1991, Fowler NEJM 2006 , Korzeniowski Ann Intern Med 1982
Echocardiography for Staph. aureusBacteremia (SAB) • Generally recommended for all patients with SAB • Approx. 20% of all comers will have evidence of endocarditis • Compliance is low • TEE vs TTE? • TTE may be adequate in low risk patients • Uncomplicated, prompt conversion of blood cultures to negative, no embolic phenomenon, no prosthetics/pacemaker, high quality study • Echo may not needed in low risk patients with • Nosocomial bacteremia (prevalence of endocarditis 4-9%) AND no hemodialysis Lancet ID 11:208, 2011; Clin Infect Dis 53:31, 2011
Vancomycin Dosing and Monitoring Vancomycin 15-20 mg/kg (actual body weight) every 8-12 hours in patients with normal renal function1(AIII). For patients with serious infections (e.g. bacteremia, endocarditis, osteomyelitis, meningitis, pneumonia), target trough concentrations of 15-20 g/mL1(BIII). Higher vancomycin doses may be associated with increased nephrotoxicity; careful monitoring is recommended.2 Trough levels should be obtained just prior to the next dose at steady state conditions (before the 4th dose) (BII). 1Rybak M Am J Health Syst Pharm 2009; Moise-Broder PA ClinPharmacokinet 2004; Jeffres MN Chest 2006; 2Jeffres MN ClinTher 2007; Lodise T AAC 2008
Management of MRSA Bacteremia and Endocarditis Vancomycin ordaptomycin 6 mg/kg IV once daily(AII) Daptomycin is noninferior to vancomycin + gentamicin1 Some experts recommend daptomycin 8-10 mg/kg IV once daily2(BIII). Doses of up to 12 mg/kg for 2 wks safe in healthy volunteers3 Clinical trial underway to further evaluate safety and efficacy 1Markowitz N Annals of Internal Med 1991; Fowler VG NEJM 2006; 2Cunha BA Heart Lung 2006; Cunha BA Heart Lung 2008; 3Benvenuto M AAC 2006 4Ardura MI PIDJ 2007
Duration of Therapy: S. aureus Bacteremia Clin Infect Dis 49:1, 2009; Clin Infect Dis 52:285, 2011
MRSA Bacteremia and Endocarditis: Role of Combination Therapy? Addition of gentamicin is not recommended for bacteremia or native-valve endocarditis (AII). No clear evidence of benefit Increased risk of nephrotoxicity1 Addition of rifampin is not recommended for bacteremia or native valve endocarditis (AI). No clear evidence of benefit2 Increased risk of drug interactions and development of rifampin resistance3 1Rybak MJ AAC 1990; Goetz, MJ JAC 1993; Rybak MJ AAC 1999; Cosgrove SE CID 2009 2Levine D Annals of Intern Med 1991; Riedel DJ AAC 2008; 3Riedel DJ AAC 2008
Thank you! • Thanks to Henry Chambers and Catherine Liu of UCSF for sharing multiple slides for this talk. phillip.coffin@sfdph.org