Download
1 / 17
180 likes | 674 Views
MRSA. Barbara Kilian, MD St.Luke’s Roosevelt Academic Associate Program Fall 2005. Study Design. Prospective Observational. The point. Quantitatively and qualitatively characterize the presentation of skin infections caused by MRSA CA-MRSA HA-MRSA. Staphylococcus Aureus. Normal flora

E N D
MRSA Barbara Kilian, MD St.Luke’s Roosevelt Academic Associate Program Fall 2005
Study Design • Prospective • Observational
The point • Quantitatively and qualitatively characterize the presentation of skin infections caused by MRSA • CA-MRSA • HA-MRSA
Staphylococcus Aureus • Normal flora • Infections • Skin/Soft Tissue • Pneumonia • Scalded Skin
Staph Aureus Gram stain “Gram positive cocci in clusters”
Infections Pneumonia
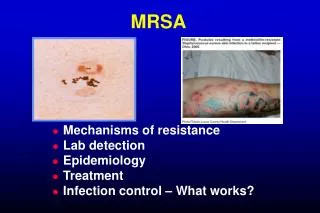
Infections cellulitis
Infections Boils
Why bother with the study? • MRSA is more prevelant • It doesn’t respond to normal ABX • Few studies done aren’t great
Methicillin-Resistant Staphylococcus aureus Disease in Three CommunitiesScott K. Fridkin, M.D., Jeffrey C. Hageman, M.H.S., Melissa Morrison, M.P.H., Laurie Thomson Sanza, R.N., Kathryn Como-Sabetti, M.P.H., John A. Jernigan, M.D., Kathleen Harriman, Ph.D., Lee H. Harrison, M.D., Ruth Lynfield, M.D., Monica M. Farley, M.D., for the Active Bacterial Core Surveillance Program of the Emerging Infections Program Network • Background Methicillin-resistant Staphylococcus aureus (MRSA)infection has emerged in patients who do not have the establishedrisk factors. The national burden and clinical effect of thisnovel presentation of MRSA disease are unclear. • Methods We evaluated MRSA infections in patients identifiedfrom population-based surveillance in Baltimore and Atlantaand from hospital-laboratory–based sentinel surveillanceof 12 hospitals in Minnesota. Information was obtained by interviewingpatients and by reviewing their medical records. Infectionswere classified as community-acquired MRSA disease if no establishedrisk factors were identified. • Results From 2001 through 2002, 1647 cases of community-acquiredMRSA infection were reported, representing between 8 and 20percent of all MRSA isolates. The annual disease incidence variedaccording to site (25.7 cases per 100,000 population in Atlantavs. 18.0 per 100,000 in Baltimore) and was significantly higheramong persons less than two years old than among those who weretwo years of age or older (relative risk, 1.51; 95 percent confidenceinterval, 1.19 to 1.92) and among blacks than among whites inAtlanta (age-adjusted relative risk, 2.74; 95 percent confidenceinterval, 2.44 to 3.07). Six percent of cases were invasive,and 77 percent involved skin and soft tissue. The infectingstrain of MRSA was often (73 percent) resistant to prescribedantimicrobial agents. Among patients with skin or soft-tissueinfections, therapy to which the infecting strain was resistantdid not appear to be associated with adverse patient-reportedoutcomes. Overall, 23 percent of patients were hospitalizedfor the MRSA infection. • Conclusions Community-associated MRSA infections are now a commonand serious problem. These infections usually involve the skin,especially among children, and hospitalization is common.
Our Study • Incision & drainage of ALL abscesses • Culture ALL of these • Follow up • Screen for ‘risk factors’
Risk Factors for HA-MRSA • Hospitalized w/in last year • Surgery w/in last year • Dialysis w/in last year • Resided in long-term care facility w/in last year • Permanent device • Positive culture in past for MRSA • ABX >3 times w/in past year • Close proximity to person with abscess/skin inf. • Has every had an abscess • DM • Injection drug use
For CA-MRSA • Sports activity • Crowded living conditions • Recurrent skin disease • “Spider” bite or other insect bite
I still don’t get what the fuss is about…. • Resistant to normal therapy • Recurrance • Exposure of others. • Leads to further resistance.