Download
1 / 48
640 likes | 1.37k Views
MRSA. Mechanisms of resistance Lab detection Epidemiology Treatment Infection control – What works?. MRSA. mec determinant >30 kb transposon mec gene approx 2.5 kb on transposon with regulatory genes and insertion sequences for other antibiotic resistance. MRSA.

E N D
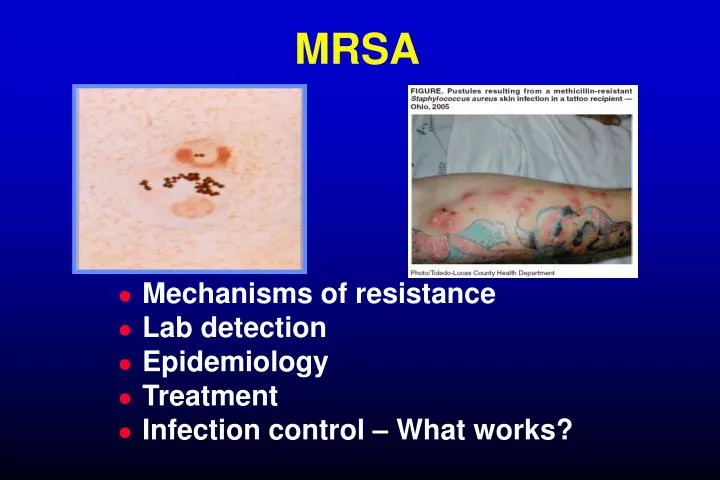
MRSA • Mechanisms of resistance • Lab detection • Epidemiology • Treatment • Infection control – What works?
MRSA • mec determinant >30 kb transposon • mec gene approx 2.5 kb on transposon with regulatory genes and insertion sequences for other antibiotic resistance
MRSA • mecA encodes a unique PBP (PBP2’ or PBP2a) with low affinity for ß-lactams, and able to fulfill functions of other PBPs • cross-resistance to all ß-lactams • heterogeneous resistance with variable expression of resistance (proportion of pop’n: 10-2-10-8)
MRSA • regulatory genes:mecI - inhibits mecAmecR1 – inducer of mecA • most MRSA have deletions orpoint mutations in mecI and mecR1 promoter regions, resulting in constitutive expression of mecA
mecImecR1mecA repressor penicilin-binding structural genes proteins signal transducer mecAPBP2a (senses presence of substrate to turn off mecI, and thereby activate mecA)
Staphylococcal Cassette Chromosome (SCC)mec SCCmec= a mobile genetic element (22-100 kb) located on chromosome; contains mecA and insertion sites (for multidrug resistance determinants) SCCmec= mec gene complex (mecI, mecR1, mecA) + ccr gene complex (ccrA, ccrB) (responsible for mobility and insertion of the gene complex) + other transposons, plasmids
SCCmec multiclonal model of evolution of MRSA: introduction of SCCmec into severalS. aureus clones
MRSALab Detection • disk diffusion: cefoxitin disk preferable to oxacillin because greater expression of mecA • oxacillin agar screen (MH agar with 4% NaCI, 6 µg/ml ox, 35ºC, 24 hrs) • broth microdilution (MH broth with 2% NaCI, 35ºC, 24 hrs;ox MIC 4 µg/ml)
MRSA Identification • detection of mecA gene (PCR) • detection of PBP2a(latex aggultination)
Prevalence of MRSA 2006 Grundmann, Lancet 2006
Prevalence of S. aureusNasal Colonization, 2003-04 National Health and Nutrition Examination Survey(NHANES) 2001-2004. Gorwitz, J Infect Dis 2008
Antibiotic Resistant Pathogensin ICU Patients (NNIS) • 29% VRE MRSA • 59% MRSE 89% 6% ESBL-E. coli • 21% ESBL-Klebsiella Quinolone-R P.aeruginosa • 30% % resistance: 1998-2002; 2003
MRSA in Canada, 1995-2008 Canadian Nosocomial Infection Surveillance Program
MRSA Infections (32%) % Canadian Nosocomial Infection Surveillance Program
MRSABloodstream Infections * Jeyaratnam, BMJ 2008; †QMPLS, 2009; § Institut National de Santé Publique du Québec, 2008
MRSA in Canada, 2008 There were: approx 32,000 new MRSA patients 13,000 new MRSA infections 2,400 MRSA-related deaths at least $250 million excess costs attributable to MRSA
MRSA in CanadaAcquisition Canadian Nosocomial Infection Surveillance Program
Molecular Epidemiology of CA-MRSA Otter, Lancet ID, 2010
MRSA in Canada:Evolving Molecular Epidemiology Simor, Infect Control Hosp Epidemiol 2010; Simor, IDSA 2010
Community-Associated MRSA • no established health care-associated risk factors: • MRSA identified >48 h after hospital admission • history of hospitalization, surgery, or dialysis within 1 yr of MRSA culture • residence in a LTCF within 1 yr of MRSA culture • indwelling catheter or device (eg. Foley catheter, tracheostomy, gastrostomy) at time of culture • prior known MRSA Naimi, JAMA 2003Fridkin, NEJM 2005
CA-MRSAPatient Profile • often younger • IVDU, MSM • incarcerated, homeless • sports teams • native aboriginals Groom, JAMA 2001; Pan, CID 2003; Naimi, JAMA 2003; Begier, CID 2004; Kazakov, NEJM 2005
Emergence of CA-MRSA as a Cause of Healthcare-Associated Infections • USA400 post-partum infections, NY (mastitis, cellulitis, abscesses) (Saiman, CID 2003) • USA300 prosthetic joint infections, Atlanta, GA (Kourbatova, Am J Infect Control 2005) • USA300 accounted for 28% healthcare-associated bacteremias, 20% nosocomomial MRSA BSIs, Atlanta, GA (Seybold, CID 2006) • USA300 common cause of SSI, University of Alabama (Patel, J Clin Microbiol 2007)
CA-MRSAVirulence • USA 300/400 more virulent than other strains of S. aureus/MRSA in a mouse model of bacteremia • more resistant to killing by human PMNs Voyich, J Immunol 2005
CA-MRSAVirulence Enhanced virulence may be related to: • global gene regulators (agr, sarA) may upregulate expression of virulence genes • acquisition of additional virulence genes
CA-MRSAVirulence • Panton-Valentine Leukocidin (PVL) • -hemolysin (increased expression in CA-MRSA; -hemolysin antibody protective in mouse model) (Wardenburg, Nature Med 2007) • Argenine catabolic mobile element (ACME;unique to CA-MRSA, S. epidermidis; may help strain evade host response and facilitate colonization)
Panton-Valentine Leukocidin • Panton-Valentine Leukocidin (PVL) • cytolytic, forms pores in human leukocytes • lukSPV-lukFPV: phage mediated • common in CA-MRSA (up to > 95%) • rare in HA-MRSA (0-1%), MSSA (5%) • associated with necrotizing pneumonia Dufour, Clin Infect Dis 2002; Diep, PLoS One 2008; Li, PNAS 2009
PVL and Survival, S. aureus Pneumonia Gillet, Lancet 2002
MRSAImpact • attributable mortality and morbidity(Whitby, Med J Austr 2001; Cosgrove, Clin Infect Dis 2003) • prolonged hospital length of stay(Engemann, Clin Infect Dis 2003; Cosgrove, Infect Control Hosp Epidemiol 2005) • excess/attributable costs, $14,360(Kim, Infect Control Hosp Epidemiol 2001)
Why does antibiotic resistance affect outcome? • Host factors • Organism virulence • Delay in instituting effective therapy (or vancomycin less effective) Bradley, Clin Infect Dis 2002; Paterson, Clin Infect Dis 2004; Kim, Antimicrob Agents Chemother 2008
Standard Treatment of MRSA Infections • source control; remove infected catheters, devices • vancomycin • other agents: clindamycin, TMP-SMX, tetracyclines, rifampin, fusidic acid
Vancomycin • less rapidly bactericidal • less effective in clinical trials (Kim, Antimicrob Agents Chemother 2008) • more toxic • may induce resistance
Vancomycin-Resistant S. aureus • 11 cases in US (2010); all MRSA, not epidemiologically linked (MI, PA, NY) • vancomycin MICs: 16 (µg/ml); vanA+ • associated with prior vancomycin exposure and VRE colonization Sievert, Clin Infect Dis 2008
VISA: Vancomycin-Intermediate • abnormal, thickened bacterial cell wall, not normally cross-linked, and with altered PBPs (no van genes) • strains appear to be clonally related (agr II group)
Vancomycin MICs and Treatment Outcome in MRSA Bacteremia p=0.003 p=0.01 1 Sakoulas, J Clin Microbiol 20042 Moise-Broder, Clin Infect Dis 2004
Predictors of Persistent MRSA Bacteremia (multivariate analysis) Yoon, J Antimicrob Chemother 2010
What about hVISA? • hVISA (heteroresistant): MIC susceptible (< 4 µg/ml), but with a resistant sub-population; detected by PAP-AUC • preliminary step towards development of VISA (Hiramatsu. Lancet ID, 2001) • may be associated with treatment failure (Sakoulas, Antimicrob Agents Chemother 2005)
Canadian MRSA and Vancomycin Adam, Antimicrob Agents Chemother 2010
Newer Antimicrobial Agents for the Treatment of MRSA • Linezolid • Daptomycin • Tigecycline • Dalbavancin, Telavancin, Oritavancin • Ceftobiprole, Ceftaroline • Iclaprim (a diaminopyramidine)
Contact Precautions Work to Decrease MRSA Transmission Jernigan, Am J Epidemiol 1996
Active Surveillance to Control Spread of MRSA • Active surveillance – finding asymptomatic carriers • Contact precautions for patients identified as colonized/infected
Evidence for Effectiveness of Active Surveillance + Contact Precautions • ecological studies (Verhoef, EJCMID 1999; Tiemersma, Emerg Infect Dis 2004) • observational/quasi-experimental studies (Jernigan, Am J Epidemiol 1996; Chaix, JAMA 1999; Huang, Clin Infect Dis 2006; Robicsek, Ann Intern Med 2008) • mathematical models (Bootsma, PNAS 2006)
Healthcare-Associated MRSA Bacteremia Rates Huang, Clin Infect Dis 2006
Controlling MRSA with Broad-Based Infection Control Interventions Edmond, Am J Infect Control 2008
MRSA:The Dutch Experience • national “search and destroy policy” screening patients, staff strict isolation decolonization environmental cleaning outbreak control Verhoef, EJCMID 1999; van Trijp, Infect Control Hosp Epidemiol 2007
MRSA in France – A Success Story Coignard, 5th Decennial International Conference on Healthcare-Associated Infections 2010 (abstr. 410)
MRSA Bacteremia - England Pearson, J Antimicrob Chemother 2009