Download
1 / 21
210 likes | 559 Views
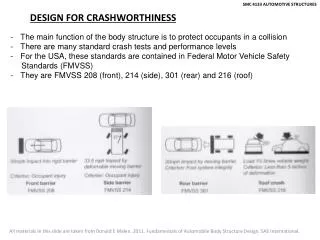
Aural Rehabilitation CDIS 4133. JACQUE SCHOLL, AU.D, CCC-A, FAAA DOCTOR OF AUDIOLOGY. AR for children. Principles of Intervention for Infants and Toddlers with hearing loss Impact of development EI Accessing the Speech Signal AR Programming Communication Modality Medical Intervention.

E N D
Aural RehabilitationCDIS 4133 JACQUE SCHOLL, AU.D, CCC-A, FAAA DOCTOR OF AUDIOLOGY
AR for children Principles of Intervention for Infants and Toddlers with hearing loss Impact of development EI Accessing the Speech Signal AR Programming Communication Modality Medical Intervention
Impact on Development Early infancy Mother-infant “courtship dance” Synchronous vs. asynchronous communication Hearing loss affects every aspect of psychological development in a bidirectional way: Social-emotional Language cognitive
Social-Emotional Development From Parent’s Perspective Parental grieving Parents may not make necessary adjustments to communication Increased control In communication In behaviour What is the impact of this increased control on the child?
Social-Emotional Development From the child’s perspective Inability to predict what will happen next Resulting frustration Fear of taking risks (e.g. new settings, new experiences) Increased dependence on others Sense of isolation and loneliness Preference for peers with same hearing status
Impact on Language Development From the Parent’s Perspective Lack of expected response Spirals of increasing control Difficulty with turn-taking Increased use of directions, 2-choice questions, “air time”
Language Impact on Development From the child’s perspective May be delayed, but not deviant Approx 1/3 of deaf children have other disabilities (leading to possible language disorder) Inability to divide attention between visual and auditory cues Strong reliance on visual cues
Each Child’s Unique Path Language development includes: Neurologically, there are many paths to language development Focus on the process; don’t worry is the path is unique
Impact on Cognitive Development A learning cycle has been created: The child does not respond as expected The parent reacts by taking control The child has less room to take risks, unless she does so quickly
Assessing Needs Determine if the child needs help Design an appropriate plan Monitor change in child and family to determine if intervention is resulting in positive outcomes
Birth to Three Mission To strengthen the capacity of families to meet the developmental and health related needs of their infants and toddlers who have hearing loss
Infant Intake Refer NBHS 1-3-6 Simultaneous: Ped Audiologist & EI enrollment Coordinated comprehensive services Collaborative partnerships Family centered Natural settings (for the most part) Best practice in EI Mutual respect for choice Develop Individualized Family Service Plan (IFSP) All services (speech/auditory dev/assistive tech) Goals and objectives Timelines
Toddler Intake Assess what language systems surround the child? What is the child’s preferred modality? Are there idiosyncracies in the child’s use of the language system? Look at the following: Age of dx Child-caregiver interactions Listening Play Vocalizations/speech/gestures Vocabulary development Combining of words/signs pragmatics
Special Considerations Formal and informal assessments are needed Most formal tests are normed on hearing children Use the child’s preferred language and receive inpt from informants across contexts For non-English speaking hearing parents, use culturally sensitive interpreters and at least one parent report instrument that is valid for the home
Principles of Intervention for all Infants and Toddlers Early identification and diagnosis is essential Ongoing audiological assessment and management must be conducted by staff trained to work with infants and young children The team should assist the family in learning about the nature of their child’s hearing loss The family is the most important member of the intervention team and information should be shared in an unbiased manner.
continued Parents and children are partners in communication. Language development begins as soon as a child is born and develops through interactions with the family in daily routines. Parents need to understand and manage the hearing aids and/or auditory equipment for their child. Parents are advocates for their child who is deaf. They need to be advised of their legal rights.
Pediatric amplification Amplify as soon as possible Select, fit and validate amplification within the first few months Real ear measures Use functional measures of benefit Scheduling flexibility Provide full access to speech (or the closest possible)
AR Programming Use of residual hearing Detection to discrimination Integrated approach Speech perception/production Language/communication Parent education Amplification Listening environment Facilitating language acquisition
Communication Modality Spoken language options AVT Cued speech Total communication Signing exact English Seeing Essential English ASL
Medical Intervention Hearing aid fitting is dependent on medical status of auditory system - Pediatric ENT Medical status of patient - PCP or other specialists Middle Ear Pathology Cochlear Implant candidacy Opthamology Genetics PT/OT/SLP/Social Work/Behavior Specialist/Teacher of the Deaf and HOH
Baby X Referred NBHS Dx at 8 months old NICU x 2 months - preemie Medically fragile State insurance Transportation is difficult - one car Frequently misses appts Mom is unable to get baby’s hearing aids in Mom wants her child to speak and listen A A X A A X X X X X