Download
1 / 67
670 likes | 824 Views
Pain. (relates to Chapter 9, “Pain,” in the textbook). Andrew. 25 y.o. male One day post op abdominal surgery You enter his room and find him smiling, joking, talking with visitor BP: 120/80; HR = 80; RR = 18 Rates his pain at 8/10. Andrew. Write what you believe is Andrew’s pain level

E N D
Pain (relates to Chapter 9, “Pain,” in the textbook)
Andrew • 25 y.o. male • One day post op abdominal surgery • You enter his room and find him smiling, joking, talking with visitor • BP: 120/80; HR = 80; RR = 18 • Rates his pain at 8/10
Andrew • Write what you believe is Andrew’s pain level • (Scale 0 = no pain; 10 = worst pain) • 0 1 2 3 4 5 6 7 8 9 10 • Write what you will document as Andrew’s pain level in his chart • (Scale 0 = no pain; 10 = worst pain) • 0 1 2 3 4 5 6 7 8 9 10
Andrew You gave morphine 2 mg IV 2 hours ago After injection, you assess his pain Q 30 minutes. Results: pain intensity 6-8 out of 10 No respiratory depression, no sedation, no side effects from morphine He has identified 2 out of 10 as an acceptable level of pain relief The order: Morphine 1 - 3 mg every hour as necessary for pain relief. What will you do? a) Administer no morphine at this time b) Administer morphine 1 mg IV now c) Administer morphine 2 mg IV now d) Administer morphine 3 mg IV now
Robert • 25 y.o. male • One day post op abdominal surgery • You enter his room. He is: lying quietly in bed, grimaces as he turns in bed • BP: 120/80; HR = 80; RR = 18 • Rates his pain at 8/10
Robert • Write what you believe is Andrew’s pain level • (Scale 0 = no pain; 10 = worst pain) • 0 1 2 3 4 5 6 7 8 9 10 • Write what you will document as Andrew’s pain level in his chart • (Scale 0 = no pain; 10 = worst pain) • 0 1 2 3 4 5 6 7 8 9 10
Robert You gave morphine 2 mg IV 2 hours ago After injection, you assess his pain Q 30 minutes. Results: pain intensity 6-8 out of 10 No respiratory depression, no sedation, no side effects from morphine He has identified 2 out of 10 as an acceptable level of pain relief The order: Morphine 1 - 3 mg every hour as necessary for pain relief. What will you do? a) Administer no morphine at this time b) Administer morphine 1 mg IV now c) Administer morphine 2 mg IV now d) Administer morphine 3 mg IV now
Discussion re Case Scenarios • Except for behaviors – both cases were identical • Subjective nature of pain – must accept patients’ reports • Multiple ways of coping with pain – laughter and distraction are common (i.e. Andrew) • Even if we may not believe a patient is not experiencing pain, we have no right to impose our beliefs on patients • Better to be “duped” than provide inadequate pain relief and nursing care • Both Andrew and Robert should receive 3 mg IV now (clearly the previous dose was not sufficient, thus it needs to be increased)
Discussion from McCaffery • Clock watchers • Other “suspect” behaviors
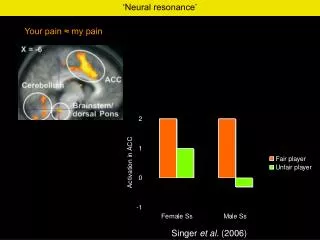
Pain • Whatever the person experiencing the pain says it is, existing wherever the person says it does (McCaffery) • An unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage
Pain • A major reasons for seeking health care • Nurses have a central role in pain assessment and management
Pain • A subjective experience • Patient’s experience and self-report is essential • Self-report can be problematic when dealing with special populations • Nonverbal information such as behaviors can also aid the assessment of pain
Nursing Roles • Assessing pain and communicating this information to other health care providers • Ensuring the initiation of adequate pain relief measures • Evaluating the effectiveness of these interventions
Nociception • Nociception is the activation of the primary afferent nerves with peripheral terminals (free nerve endings) that respond differently to noxious (tissue-damaging) stimuli • Nociceptors function primarily to sense and transmit pain signals
Dimensions of Pain Affective (emotions, suffering) Physiologic (transmission of nociceptive stimuli) Behavioral (behavioral responses) PAIN Cognitive (beliefs, attitudes, evaluations, goals) Sensory (pain perception) Fig. 9-1
Mechanism by Which Pain is Perceived Fig. 9-2
Medications Interrupt the Pathway • Transduction (e.g., NSAIDS, local anesthetics) • Transmission (e.g., opioids) • Perception (e.g., opioids, adjuvants, NSAIDS) • Modulation (e.g., tricyclic anti-depressants)
Classification of Pain • Acute • Chronic
Acute Pain • Sudden onset • < 3 months or as long as it takes for normal healing to occur • Mild-to-severe pain • Generally can identify a precipitating event or illness (e.g., surgery)
Acute Pain • Course of pain ↓ over time and goes away as recovery occurs • Includes postoperative pain, labor pain, pain from trauma • Treatment includes analgesics for symptom control and treatment of the underlying cause
Acute Pain • Manifestations reflect sympathetic nervous system activation • ↑ heart rate • ↑ respiratory rate • ↑ blood pressure • Pain control with eventual elimination is treatment goal
Chronic Pain • Gradual or sudden onset • > 3 month duration; may start as acute injury or event but continues past the normal recovery time • May not know cause of pain
Chronic Pain • Typically pain does not go away; characterized by periods of waxing and waning • Mostly behavioral manifestations • ↓ physical movement/activity • Fatigue • Withdrawal from others and social interaction
Chronic Pain • Can be disabling and is often accompanied by anxiety and depression • Treatment goals • Pain control to the extent possible • Focus on enhancing function and quality of life
Assessment of Pain: PQRST P = Provoking/Palliating factors • What precipitates/provokes the pain? What makes it worse? • What makes it better (palliates)? Q = Quality • What does it feel like? Ask open-end questions. R = Region/radiation • Where is the pain? Does it travel or radiate?
Assessment of Pain: PQRST S = Severity • VAS (Visual analogue scale) • Numerical scale (0 - 5; 0 - 10) • Descriptive scale (no pain, mild, moderate, severe, very severe, worst possible) • FACES pain rating scale - for children, non-verbal, language barriers T = Time/temporal factors • When did it begin? How long does it last? When does it occur? Does it come and go? Is it constant?
Assessing Pain in Cognitively Impaired/Non-verbal Adults • Self-report whenever possible: Often can use numerical scales if taught 0 - 5 scale may be easier Faces scale - 6 different facial images
Assessing Pain in Cognitively Impaired/Non-verbal Adults • Alternatives to self-report (from most to least useful) • Pathologic conditions or procedures known to cause discomfort • Behaviors • Facial expressions (frown, grimace, contract muscles around mouth/eyes) • physical movements (restless, fidget, resists movement, guarding, combativeness, hostile behavior) • Vocalizations (moan, groan, crying) • Proxy pain rating (family, friends, clinician) - only a guess • Physiological Measures (e.g., HR, RR, BP- elevated) - least helpful
Points to Remember: Special Considerations • Prevalence of pain increases with age • Pain is most under-treated among elderly • No reason to believe that age or cognitive impairment dulls sensitivity to pain • Make sure patient can see/use assessment tool (glasses, hearing aid, teach)
Factors affecting expression of pain • Age • pain wrongly accepted as part of aging • sign of weakness • don’t want to bother nurse • Gender • pain experience/perception may be different between genders • belief that men should be more stoic • Cultural Influences • Cause of pain (fate, lifestyle, punishment, witchcraft) • Emotional response and expression • Meaning of pain • Reports of intensity • How it should be treated/who treats it
Why People Deny Pain • Fear of Addiction • Discuss this common fear • Emphasize rarity of addiction when opioids used for pain (< 1%) • Fear of Developing Tolerance • Fear analgesic might not work when really needed • Emphasize can increase dose
Why People Deny Pain • Fear of Side Effects • Teach can treat and/or prevent these • Desire to be good patient/non-complainer • Explain importance of pain relief in preventing complications • Fear of Showing Weakness • Explain importance of pain relief for quality of life, maintaining control of life
Indicators of Denial of Pain • Known painful condition/procedure • Pain behaviors (grimacing, guarding, etc.) • Family/friends suspect pain • If denial suspected • Identify concerns and discuss • Ultimately, must accept patient’s self-report
Despite the prevalence of pain, many studies document inadequate pain management across care settings and patient populations
Consequences of Untreated Pain • Unnecessary suffering • Physical and psychosocial dysfunction • Impaired recovery from acute illness and surgery • Immuno-suppression • Sleep disturbances
Reasons for Under-Treatment of Pain • Inadequate professional knowledge • MDs under-prescribe; nurses under-administer • Fear of addiction by patients and practitioners • Lack of knowledge re difference between physical dependence, tolerance, addiction
Reasons for Under-Treatment of Pain • Inadequate assessment techniques • Inadequate use of assessment tools • Inadequate evaluation of effects of analgesia • Hesitance to believe self-reports • Lack of knowledge re cultural differences in pain expression • Pain management not a priority
Reasons for Under-Treatment of Pain • Inadequate Consumer knowledge • That most pain can be relieved • Fear of addiction/tolerance
Reasons for Under-Treatment of Pain • Communication Problems • Professionals • Not a priority • May not impress upon patients importance of achieving adequate pain control (reduces post-op complications, reduces hospital LOS, etc) • Consumers • Desire to be “good” patient; don’t want to “bother” nurse • Cultural variations in expression
Physical Dependence • May develop after using opioids for 1-4 weeks or longer • If opioid stopped or antagonist is taken/given, withdrawal symptoms (mild-severe) occur • Yawning, chills, GI upset, tearing of eyes • May progress to muscle spasms, vomiting, diarrhea
Tolerance • May develop after using opioids for 1-4 weeks or longer • Characterized by reduced effect of the opioid: • Reduced pain relief • Decrease in side effects, such as nausea, sedation, itching, or respiratory depression • Treat by increasing dose
Addiction • Psychological dependence • Compulsive drug use • Continued craving • Opioids needed for other than pain relief • An acquired disease of brain • Rarely occurs when opioids used for pain relief • Of 24,000 patients whose pain was treated with opioids, < 1% became addicted (7 of 24,000 patients) • Fear of addiction is never a reason to withhold opioids from patients in pain
Pain Management and Substance Abusers • Discuss McCaffery
Pain Treatment • All pain treatment is guided by the same underlying principles • The patient must always be believed • Every patient deserves adequate pain management • Set goals for comfort and function - e.g., what pain rating would allow patient to do post-op recovery activities? - generally ratings > 3-4 interferes with function
Pain Treatment • Prevent occurrence and recurrence - Predictable pain - give analgesic before - Pain around the clock (ATC) – analgesics ATC (wake patient for analgesic before the pain wakes patient) • All therapies must be evaluated to ensure they are meeting patient’s goals
Drug Therapy • Non-opioids • Opioids • Adjuvents Each works on pain in different ways (interrupt pathways in different points/ways), so can combine different types for maximal pain relief
Drug Therapy • See WHO Analgesic Ladder for management of pain (p. 142) • See Equi-analgesic chart (McCaffery)
Non - Opioids Acetaminophen and NSAIDS • General purpose analgesics • Acute and chronic pain • Especially for mild MS pain • Also used in combination with adjuvants and opioids for moderate - severe pain • Have a ceiling effect - no more pain relief will be obtained beyond a certain dose
Non-Opioids • Acetaminophen (i.e., Tylenol) • Analgesic action appears to be in CNS • Safest non-opioid for most patients, especially elderly • Does not increase bleeding time or cause ulcers • May cause hepatotoxicity (do not use in chronic liver disease or alcoholism) • Maximum daily dose: 4000 mg • Also an anti-pyretic (for fever) • Not an anti-inflammatory; not anti-platelet
Non-Opioids • NSAIDS • ASA/Aspirin, Ibuprofin/Motrin/Advil, Celebrex, Vioxx • Relieve pain at site of injury and act on CNS • Block prostaglandin production at site of injury • When NSAID doesn’t work: increase dose or try another type • NSAIDS are also • anti-inflammatory • anti-pyretics (for fever) • anti-platelet (prevent clotting)