Download
1 / 26
290 likes | 407 Views
Part 2.0 Standardised Interpretation of Paediatric CXR. Done in collaboration with: The Northern School of Radiology, UK County Durham and Darlington NHS Foundation Trust Authors : Dr . Alasdair Mackie MD Dr . Nadia Mcallister MD Dr . Abdelrahman Omer MD Dr. Ramdas Senasi MD

E N D
Part 2.0Standardised Interpretation of Paediatric CXR Done in collaboration with: The Northern School of Radiology, UK County Durham and Darlington NHS Foundation Trust Authors: Dr. Alasdair Mackie MD Dr. Nadia Mcallister MD Dr. Abdelrahman Omer MD Dr. Ramdas Senasi MD Special Thanks: Professor Bernard Laya
Aim • Demonstrate a systematic approach to paediatric Chest X-rays using an ABCDE method.
Systematic approach Technique • A - Airways and lungs • B - Bones and soft tissues • C - Cardiac • D - Diaphragm • E - Extra body equipment • + - ABC Double check: Important review areas to minimise missing abnormalities.
Technique • RIPE • Rotation • Inspiration • Picture • Exposure Centred film. Equal distance between medial ends of clavicles
Technique • RIPE • Rotation • Inspiration • Picture • Exposure Rotated film. Note the gap between medial end of right clavicle.
Technique Normal CXR, should see 7 anterior ribs and 9 posterior. Do not need to count both. • RIPE • Rotation • Inspiration • Picture • Exposure 1 2 3 4 1 5 2 6 3 7 4 8 5 6 9 7 Posterior ribs Anterior ribs
Technique • RIPE • Rotation • Inspiration • Picture • Exposure Underinflated Overinflated
Technique Ensure important body parts included in image • RIPE • Rotation • Inspiration • Picture • Exposure Adequate CXR Suboptimal CXR
Technique Vertebral bodies should be faintly visible throughout. • RIPE • Rotation • Inspiration • Picture • Exposure Underexposed ‘too bright’ Overexposed ‘too dark’
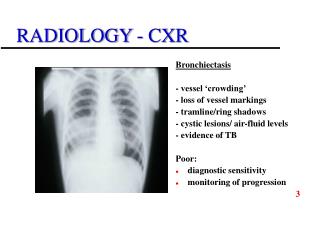
Systematic approach • Technique • Airways and lungs: • B • C • D • E • + - ABC Double check. Start at top and compare right with left. Trachea should always be central. Can deviate to right on expiration in younger patients.
Lobar anatomy – right lung – 3 lobesupper, middle and lower lobes
Systematic approach • Technique • A • Bone and soft tissues: • C • D • E • + - ABC Double check. Bony or soft tissue lesions can be easily missed if not looked for.
Abnormal soft tissue mass at right apex. Abnormal bony lesion on left rib.
Systematic approach • Technique • A • B • Cardiac and mediastinum: • D • E • + - ABC Double check. Important to review size, borders and for mediastinal masses.
Normal Normal thymus Normal thymus Mediastinum; thymus regularly seen in children. Not to be confused with mediastinal lymphadenopathy. Size; generally no more than 50% (exception is neonates, can be bigger) Abnormal mediastinal adenopathy seen in lymphoma Enlarged
Systematic approach • Technique • A • B • C • Diaphragms: • E • + - ABC Double check. Should be clear and crisp, if blurred/obscured this should raise suspicion.
Right hemi diaphragm is normally higher than the left, approximately one rib space. Clear costophrenic angles. Normal Right sided effusion. Can not see entire hemi diaphragm and have lost costophrenic angle.
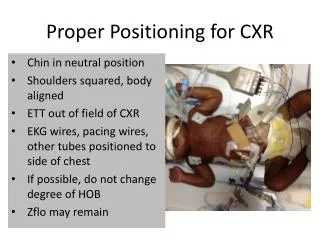
Systematic approach • Technique • A • B • C • D • Extras: • + - ABC Double check. Check for lines and tubing
Endotracheal tube Temperature probe Nasogastric tube Endotracheal tube Central line Umbilical artery catheter Nasogastric tube Umbilical vein catheter
Systematic approach • Technique • A • B • C • D • E • + - ABC Double check Apex, Behind heart, costophrenic and cardio phrenic angles.
These lesions can be easily missed. Review areas are important.
Summary • Demonstrated a systematic approach to paediatric CXR using ABCDE. • Reinforced importance of review areas to ensure subtle things not missed.
Thank you for your attention. • Any questions?
References • Images obtained from following resources; • Eurorad.org • Radiopaedia.org • Wikiradiography.net • Lifeinthefastlane.com • Slideshare.net