Download
1 / 1
20 likes | 645 Views
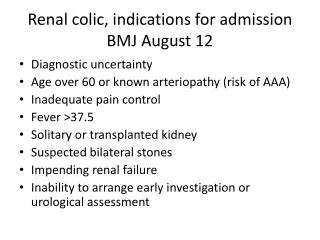
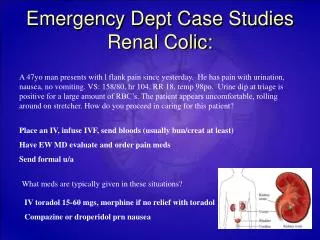
Proposed Care pathway for Renal Colic (to be developed). High risk cases needing emergency 2 nd care assessment : Solitary functioning kidney Pyrexia +/- other signs of infection (such as peritonitis) Systemically unwell (hypovolaemia) +/- oliguria/anuria

E N D
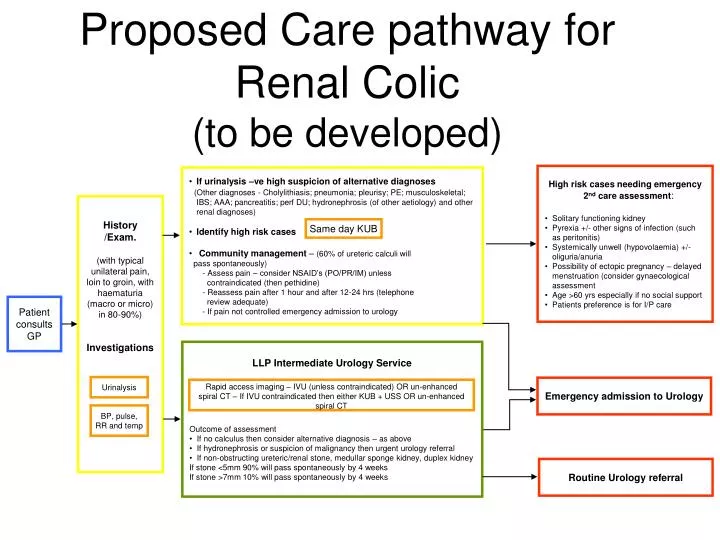
Proposed Care pathway for Renal Colic(to be developed) • High risk cases needing emergency 2nd care assessment: • Solitary functioning kidney • Pyrexia +/- other signs of infection (such as peritonitis) • Systemically unwell (hypovolaemia) +/- oliguria/anuria • Possibility of ectopic pregnancy – delayed menstruation (consider gynaecological assessment • Age >60 yrs especially if no social support • Patients preference is for I/P care • If urinalysis –ve high suspicion of alternative diagnoses • (Other diagnoses - Cholylithiasis; pneumonia; pleurisy; PE; musculoskeletal; IBS; AAA; pancreatitis; perf DU; hydronephrosis (of other aetiology) and other renal diagnoses) • Identify high risk cases • Community management – (60% of ureteric calculi will • pass spontaneously) • - Assess pain – consider NSAID’s (PO/PR/IM) unless • contraindicated (then pethidine) • - Reassess pain after 1 hour and after 12-24 hrs (telephone • review adequate) • - If pain not controlled emergency admission to urology History /Exam. (with typical unilateral pain, loin to groin, with haematuria (macro or micro) in 80-90%) Investigations Same day KUB Patient consults GP • LLP Intermediate Urology Service • Outcome of assessment • If no calculus then consider alternative diagnosis – as above • If hydronephrosis or suspicion of malignancy then urgent urology referral • If non-obstructing ureteric/renal stone, medullar sponge kidney, duplex kidney • If stone <5mm 90% will pass spontaneously by 4 weeks • If stone >7mm 10% will pass spontaneously by 4 weeks Urinalysis Emergency admission to Urology Rapid access imaging – IVU (unless contraindicated) OR un-enhanced spiral CT – If IVU contraindicated then either KUB + USS OR un-enhanced spiral CT BP, pulse, RR and temp Routine Urology referral