Download
1 / 31
390 likes | 906 Views
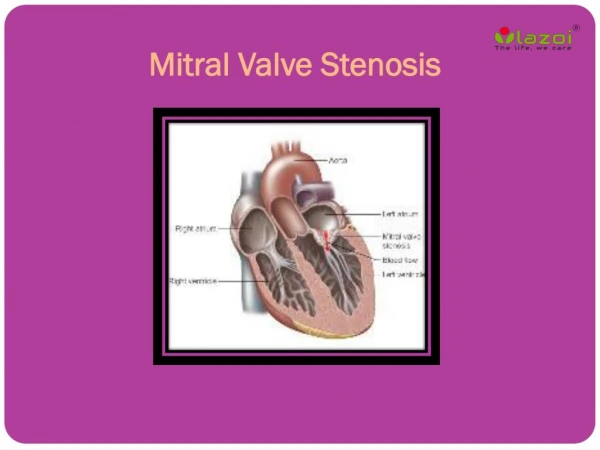
Treatment of Mitral Stenosis. Treatment of Mitral Stenosis. Medical Valvotomy Interventional Surgical. Interventional Valvotomy. Percutaneous MV Comissurotomy (PMC) Percutaneous MV Replacement ? ( new technique ). Percutaneous Mitral Valve Commissurotomy ( PMVC ).

E N D
Treatment of Mitral Stenosis • Medical • Valvotomy • Interventional • Surgical
Interventional Valvotomy • Percutaneous MV Comissurotomy (PMC) • Percutaneous MV Replacement ? ( new technique )
Percutaneous Mitral Valve Commissurotomy ( PMVC ) Balloon commissurotomy Metallic commissurotomy
Balloon Commissurotomy • Antegrade ( Teansseptal ) • Single balloon ( Inoue ) • Double balloon • Retrograde ( Transatrial )
Antegrade PMVC Most common procedure is Inoue balloon MVA become slightly more larger in double balloon catheter than Inoue balloon Risk of perforation is greater in double balloon procedure than Inoue balloon Suitable , when interatrial thrombosis is not present
Retrograde PMVC When transseptal approach is contraindicated or impossible
Metalic Commissurotomy Uses a device similar to the tubes dilator Efficacy similar to BMVC More demanding for operator than BMVC Advantage is that dilator is reusable
Indication of Valvotomy( most be individualized ) Symptomatic patients Asymptomatic patients
Indication of Valvotomy in Symptomatic Patients , if: • Sever MS ( MVA ≤ 1 cm2 ) • Moderate MS ( MVA ≤ 1.5 cm2 ) • Functional class II • PA pressure > 60 mmHg • Mean PCWP > 25 mmHg during exercise
Indication of Valvotomy in Asymptomatic Patients Women with sever MS who wish to become pregnant Who experience recurrent thromboembolie events Who have sever pulmonary hypertension Atrial fibrillation ( persistent or recurrent )
Indication of PMVC Patients who indicated for valvotomy + good MV scoring (≤ 8 )
Mitral Valve Scoring Mobility ( 1-4 ) Subvalvular thickening ( 1-4 ) Leaflet thickening ( 1-4 ) Calcification ( 1-4 )
Contraindication of PMVC • LA thrombosis • Floating in LA • Attached to interatrial septum • Severe scoliosis • IVC obstruction • Major abnormalities of interatrial septum
Advantages of BMVC Percutaneous Local anesthesia Good hemodynamic result Good long-term outcome
Disadvantages of BMVC No direct visualization of valve Only feasible with flexible & non calcified valves Contraindicated if MR> 2+ or LA clot is present
Balloon Size Patient’s height Body surface area Diameter of Mitral annulus
Complication of PMVC Cerebral emboli (1%) Cardiac Perforation (1%) Development of severe MR ( 2% need to surgery ) Residual small ASD (5%)
Surgical treatment of MS • Valvotomy • Closed MV commissurotomy ( CMVC) • Open MV commissurotomy ( OMVC ) • MV replacement • Metallic • Biologic
Closed MV commissurotoimy • Advantages : • Off pump • Inexpensive • Relatively simple • Good hemodynamic result • Good long-term outcome
Closed MV commissurotoimy • Disadvantages : • No direct visualization of valve • Only feasible with flexible / non calcified valves • Contraindicated if MR>2+ • Need to general anesthesia
Open MV commissurotoimy • Advantages : • Risk of dislodging thrombi from the atrium or calcium from valve s low • Visualization of valve allows direct valvotomy • Concurrent annuloplasty for MR is feasible
Open MV commissurotoimy • Disadvantages : • Surgical procedure with general anesthesia • Best results with flexible / non calcified valve
Indications of MVR • Combined MS + moderate to severe MR • Extensive commissural calcification • Severe fibrosis • Subvalvular fusion • Previous valvotomy • Whose valves are not suitable for valvotomy : • MVA < 1.5 cm2 + Fc III-IV • MVA < 1 cm2 + Fc II + PAP>70 mmHg
Prosthetic Mitral valve • Bioprosthetic • Mechanical : • Caged ball ( starr – Edwards) • Tilting disc: • Monoleaflet ( Bjork – shiley ) • Bioleaflet ( St. jude )
Advantage of mechanical valve durability
Disadvantage of mechanical valve • Thromboembolism • Valvular thrombus • Valvular failure • Valvular infection • Pregnancy ( none of the 3 available anticoagulants have been effective )
Off pump MVR ( new technique) • Double-crowned valved stent: • Ventricular stent ( fixation of device to the Mitral annulus ) • Atrial stent ( holds in place the homograft sutured on the prosthesis ) • The grocre between the two crowns is placed at the level of the Mitral annulus • Self-expandable artificial heart valve
Approach to off pump MVR Lt. posterolateral thoracotomy in 4th intercostal space The atrium was punctured with a needle and a guide wire was inserted into it before a short 9-F sheath was introduced Ivus was inserted in order to measure the diameter and Mitral valve area Position of annulus was confirmed as well under the guidance of fluoroscopy An incision of 1 cm was made on left atrium, centralled by the purse strings
Complication of off pump MVR Mild peravalvular regurgitation due to mismatch between native annulus + valve size LVOT obstruction due to protrusion of valved stents into the LV + push anterior of the MV towards the LVOT ( similar to SAM)
Indication of off pump MVR Patients with : • MR who no candidate for open heart surgery • Severe CHF • Hepatic failure • Renal failure • Restenosis of MV after PMC