Download
1 / 15
150 likes | 316 Views
Suppression of Bone Resorption in OI VI using the RANKL Antibody Denosumab. Heike Hoyer-Kuhn Oliver Semler / Eckhard Schoenau. ICCBH, Rotterdam, June 24th 2013. Introduction – OI VI. Characterization based on clinical / histological findings: No fractures at birth

E N D
Suppression of Bone Resorption in OI VI using the RANKL Antibody Denosumab Heike Hoyer-KuhnOliver Semler / Eckhard Schoenau ICCBH, Rotterdam, June 24th 2013
Introduction – OI VI • Characterization based on clinical / histological findings: • No fractures at birth • Fractures more frequent • Typical histomorphometric findings with mineralization defect and elevated osteoid volume
Introduction – OI VI • Patientswith OI type VI showed a reducedtreatmentresponsetopamidronatecomparedto OI type I/III/IV: • Fracturesmorefrequentdespitebisphosphonatetreatment • Reducedgrowthvelocity • Noreductionof vertebral compressions
Introduction – SERPINF1 • Member oftheserpingenefamilycodingfor PEDF (pigmentepithelderivedfactor). • SERPINF1mutationsleadtoreduced PEDF expression. • PEDF isinvolved in angiogenesisand neuronal differentiation. • In PEDF knockout mice (-/-) boneabnormalitiesarecomparabletothoseseen in patientswith OI VI. • Type I collagenproductionis normal andseems not tobeaffectedin thesepatients. Bogan et al., JBMR Jul 2013;28(7):1531-1536.
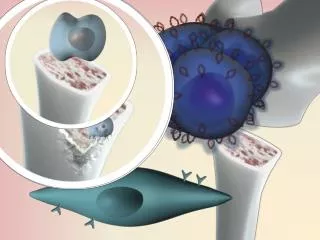
Introduction – Role of PEDF PEDF RANKL OPG SERPINF1 Modified from Boyle WJ, et al. Nature. 2003;423:337-342
Introduction - Mutation in SERPINF1 PEDF RANKL OPG SERPINF1 Modified from Boyle WJ, et al. Nature. 2003;423:337-342
Introduction - Denosumab PEDF RANKL OPG OPG Denosumab SERPINF1 Modified from Boyle WJ, et al. Nature. 2003;423:337-342
Is there a suppression of bone resorption in children with OI type VI treated with the RANKL antibody denosumab ? Research question:
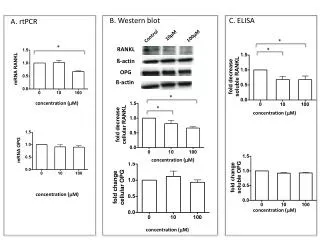
Results – osteoclastic activity Urinary DesoxyPyriDinoline (DPD)
Results - DPDs Denosumab Treatment Normal range Unpublished data
Results – arealBoneMineral Density(DXA) aBMD L2-L4 I.B., male, 10.5 years aBMD L2-L4 K.M., male, 8.5 years Z-score Z-score Start Denosumab Start Denosumab 1 0 -1 -2 -3 -4 1 0 -1 -2 -3 -4 6 7 8 9 10 11 6 7 8 9 10 11 Age (Years) Age (Years) Unpublished data
The first applications of denosumab in children with OI VI were well tolerated and showed no severe side effects. DPD levels and BMD measurement provided evidence that treatment with denosumab reduced bone resorption in OI VI. The antiresorptive treatment with denosumab should be evaluated in clinical trials to optimize intervals and to analyze its efficacy in a larger cohort of OI type VI children. Summary / Conclusion
Acknowledgements: Children`shospital Rehabilitation Human Genetics FundedbyKöhler Award 2012 HHK and OS declare no conflicts of interest. ES received speakers fee from Amgen.