Download
1 / 1
10 likes | 985 Views
Bortezomib (VELCADE), Rituximab, Cyclophosphamide, Dexamethasone (VRCD) combination therapy in front-line low-grade non-Hodgkin lymphoma (LG-NHL) is active in elderly patient population. Chadi Nabhan MD FACP, Neil Dalal DO, Kathy Tolzien RN, Alexander Starr MD

E N D
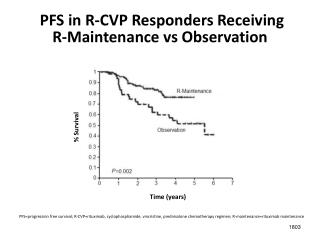
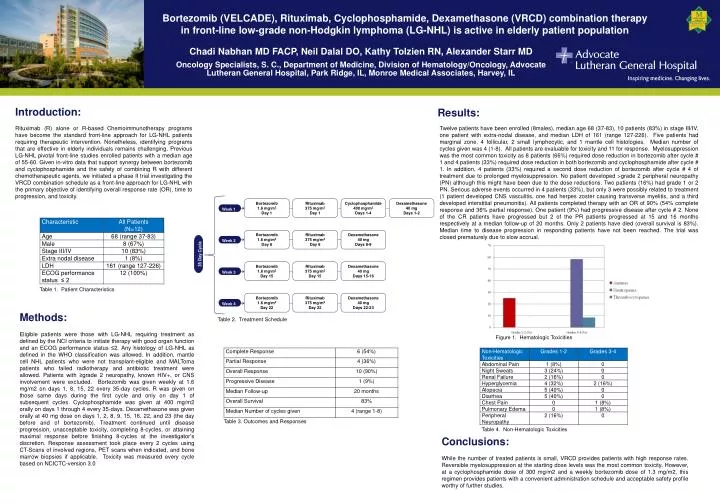
Bortezomib (VELCADE), Rituximab, Cyclophosphamide, Dexamethasone (VRCD) combination therapy in front-line low-grade non-Hodgkin lymphoma (LG-NHL) is active in elderly patient population Chadi Nabhan MD FACP, Neil Dalal DO, Kathy Tolzien RN, Alexander Starr MD Oncology Specialists, S. C., Department of Medicine, Division of Hematology/Oncology, Advocate Lutheran General Hospital, Park Ridge, IL, Monroe Medical Associates, Harvey, IL Introduction: Results: Rituximab (R) alone or R-based Chemoimmunotherapy programs have become the standard front-line approach for LG-NHL patients requiring therapeutic intervention. Nonetheless, identifying programs that are effective in elderly individuals remains challenging. Previous LG-NHL pivotal front-line studies enrolled patients with a median age of 55-60. Given in-vitro data that support synergy between bortezomib and cyclophosphamide and the safety of combining R with different chemotherapeutic agents, we initiated a phase II trial investigating the VRCD combination schedule as a front-line approach for LG-NHL with the primary objective of identifying overall response rate (OR), time to progression, and toxicity. Twelve patients have been enrolled (8males), median age 68 (37-83), 10 patients (83%) in stage III/IV, one patient with extra-nodal disease, and median LDH of 161 (range 127-226). Five patients had marginal zone, 4 follicular, 2 small lymphocytic, and 1 mantle cell histologies. Median number of cycles given was 4 (1-8). All patients are evaluable for toxicity and 11 for response. Myelosuppression was the most common toxicity as 8 patients (66%) required dose reduction in bortezomib after cycle # 1 and 4 patients (33%) required dose reduction in both bortezomib and cyclophosphamide after cycle # 1. In addition, 4 patients (33%) required a second dose reduction of bortezomib after cycle # 4 of treatment due to prolonged myelosuppression. No patient developed >grade 2 peripheral neuropathy (PN) although this might have been due to the dose reductions. Two patients (16%) had grade 1 or 2 PN. Serious adverse events occurred in 4 patients (33%), but only 3 were possibly related to treatment (1 patient developed CNS vasculitis, one had herpes zoster causing transverse myelitis, and a third developed interstitial pneumonitis). All patients completed therapy with an OR of 90% (54% complete response and 36% partial response). One patient (9%) had progressive disease after cycle # 2. None of the CR patients have progressed but 2 of the PR patients progressed at 15 and 16 months respectively at a median follow-up of 20 months. Only 2 patients have died (overall survival is 83%). Median time to disease progression in responding patients have not been reached. The trial was closed prematurely due to slow accrual. Table 1. Patient Characteristics Methods: Table 2. Treatment Schedule Bortezomib 1.6 mg/m2 Day 1 Rituximab 375 mg/m2 Day 1 Cyclophosphamide 400 mg/m2 Days 1-4 Dexamethasone 40 mg Days 1-2 Eligible patients were those with LG-NHL requiring treatment as defined by the NCI criteria to initiate therapy with good organ function and an ECOG performance status ≤2. Any histology of LG-NHL as defined in the WHO classification was allowed. In addition, mantle cell NHL patients who were not transplant-eligible and MALToma patients who failed radiotherapy and antibiotic treatment were allowed. Patients with ≥grade 2 neuropathy, known HIV+, or CNS involvement were excluded. Bortezomib was given weekly at 1.6 mg/m2 on days 1, 8, 15, 22 every 35-day cycles. R was given on those same days during the first cycle and only on day 1 of subsequent cycles. Cyclophosphamide was given at 400 mg/m2 orally on days 1 through 4 every 35-days. Dexamethasone was given orally at 40 mg dose on days 1, 2, 8, 9, 15, 16, 22, and 23 (the day before and of bortezomib). Treatment continued until disease progression, unacceptable toxicity, completing 8-cycles, or attaining maximal response before finishing 8-cycles at the investigator’s discretion. Response assessment took place every 2 cycles using CT-Scans of involved regions, PET scans when indicated, and bone marrow biopsies if applicable. Toxicity was measured every cycle based on NCICTC-version 3.0 Week 1 Figure 1. Hematologic Toxicities Bortezomib 1.6 mg/m2 Day 8 Rituximab 375 mg/m2 Day 8 Dexamethasone 40 mg Days 8-9 Week 2 35 Day Cycle Bortezomib 1.6 mg/m2 Day 15 Rituximab 375 mg/m2 Day 15 Dexamethasone 40 mg Days 15-16 Week 3 Table 3. Outcomes and Responses Table 4. Non-Hematologic Toxicities Bortezomib 1.6 mg/m2 Day 22 Rituximab 375 mg/m2 Day 22 Dexamethasone 40 mg Days 22-23 Week 4 Conclusions: While the number of treated patients is small, VRCD provides patients with high response rates. Reversible myelosuppression at the starting dose levels was the most common toxicity. However, at a cyclophosphamide dose of 300 mg/m2 and a weekly bortezomib dose of 1.3 mg/m2, this regimen provides patients with a convenient administration schedule and acceptable safety profile worthy of further studies.