Download
1 / 30
300 likes | 523 Views
The Partner Counseling and Referral Service Model. Janet Furseth, RN BN Public Health Nurse Harm Reduction Team Calgary Health Region. The PCRS Process. Pre-test Counseling. Post-test Counseling. Partner Notification. History of Partner Notification. 1930’s: “Contact Tracing”

E N D
The Partner Counseling and Referral Service Model Janet Furseth, RN BN Public Health Nurse Harm Reduction Team Calgary Health Region
The PCRS Process Pre-test Counseling Post-test Counseling Partner Notification
History of Partner Notification • 1930’s: “Contact Tracing” • Prevent spread of syphilis • Later expanded to included gonorrhea and other Sexually Transmitted Infections (STI) • 1980’s: “Partner Notification” • HIV became a Public Health issue • Sexual and needle sharing partners • Late 1990’s: “Partner Counseling and Referral Services” • Reflects the range of services offered
Unique Issue with Partner Notification and HIV Infection • lack of a drug therapy to cure HIV or prevent transmission • a long incubation period which makes it difficult for patients to name and locate past partners • serious concerns about confidentiality and social stigma.
“The medical officer of health shall ensure that an attempt is made to identify, locate and offer counseling and testing to sexual, needle sharing and perinatal contacts of the patient” Province of Alberta Public Health Act
Why Do Partner Counseling • Required, according to the Public Health Act • To identify people who may be at risk • To identify people who may be putting others at risk • Education opportunity • Decrease the incidence of HIV infection
Four Major Stakeholders in PCRs • The HIV infected clients • Their partners • The community • Health care providers
HIV Infected Client • Needs to believe in the process • People can not be coerced into providing information • Needs to be able to trust the process • Confidentiality respected • safety • Fulfills ethical responsibility to partner • Opportunity for behavior change
Partners • Education opportunity – regardless of HIV status • Early diagnosis and treatment/medical care • May perceive invasion of privacy • “Need” to know who gave their name
The Community • Reduce the burden of disease • Reduce the transmission within the community • Sense of feeling protected • Normalize testing • May be seen as intrusive
Health Care Provider • Public Health Nurse • Family Doctor • STI Clinic • Outreach worker (safeworks van) A client is more likely to disclose to a health care worker they are comfortable with/have a relationship with
The Process: essential Concepts • PCRS is voluntary • Client Centered • PCRS in ongoing • Confidential
Voluntary • Relies on the willing participation of HIV infected individual • Can not be mandatory or coercive • An atmosphere of trust must be created • Client must believe in the process
Client Centered • Focus on client’s feelings • Deal with client’s real situation • Allow individual to find their own solutions • Ensure safety (i.e. current partner) • Non judgmental
Ongoing • PCRS activities need to be offered whenever an HIV infected person accesses services (not just when 1st +) • When diagnosed with any other STI • During appointments for other health matters • When discussing family planning/ birth control • Accessing alcohol & drug counseling
Confidential • No client information will be released to partners (name, gender, type of exposure, time/location of exposure) • Health care provider may or may not know identity of case • Phone messages “Janet a nurse” • Letters/email “need to discuss a health matter” • Client is not entitle to be told results of partners • Case & partners are not linked in documentation
Four Options • Provider Option • Client Option • Dual Option • Combination Option
Provider Option • Done at request of client • Gather as much information a possible from case • anonymous
Name Address Phone number Gender Age Tattoos Piercing Scars Eye color Hair color Family contacts Friends Employer School Hang outs Car Required Partner Information
Client Option • Client takes responsibility for contact and talking partner • Health care provider provides resources, guidelines and coaching • No need to gather partner information
Dual Option • Client tells partner in presence of the health care provider • Provider is then available to address partner concerns and questions. • Confidentiality is still respected • Plan in advance how interaction will go and provide client coaching
Combination Option • Client agrees to talk with partners but if unable the health care provider will assume responsibility (confidentially) • Agree on a timeline for completion • Health care provider follows up to confirm client was able to notify partners
Time Frame • 6 months before last negative • If no negative test result – lifetime partners • More recent the contact the better the success in locating individuals • Current partners, encourage notification by client
Locating Partners • Phone • Letter • Email • “the van” • other city/provinces • Confidentiality is maintained at all times
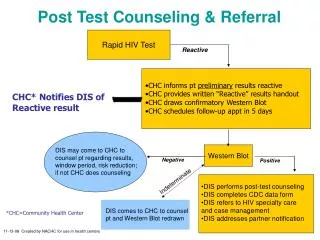
Counseling Partners • Ensure it is the right person • Private/safe area to talk • Answer questions • What is HIV • How is it spread/prevented • Direct to testing facility
Benefits of PCRS • Allows client to inform partners without revealing own HIV status • Relieves client of responsibility (legal and ethical) • Opportunity for behavior change/education • Linkage to other services • Opportunity for early diagnosis/treatment • Reduces transmission in the community
Challenges/Concerns of PCR • Threat to confidentiality • Fear of Judgment • Threat of discrimination • Intrusion on personal life • Potential for violence • Cost