Download
1 / 64
640 likes | 766 Views
Public Health Bill Workshops. PHA February 2008. PHA workshops. Help PHA make an excellent submission to Parliament Inform others about the Bill and encourage them to make submissions supportive of public health. Governments can: -. Fund things. Have staff do things. Talk up ideas.

E N D
Public Health Bill Workshops PHA February 2008
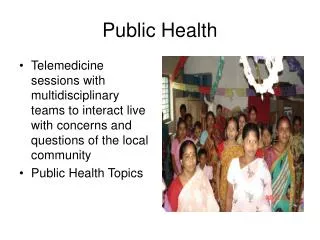
PHA workshops • Help PHA make an excellent submission to Parliament • Inform others about the Bill and encourage them to make submissions supportive of public health
Governments can: - Fund things Have staff do things Talk up ideas Pass laws
Today Pass laws
Heath Act RMA, Biosecurity, Building, HSNO, LGA TB Burials & Cremation Legal context Mental Health (CAT)
Health and disability, Medicines HPCAA H&D Commissioner Radiation Protection Health laws Health Act / PH Bill SOL, SFE GA, … Mental Health (CAT)
Act, Bills and Regulations Bill a proposed law being considered by Parliament Act a law passed by Parliament Regs further detailed laws under a specific Act, if that Act permits the making of such regulations
Achieving healthy public policy • Parliament makes or changes laws • MMP environment • We have (and have had) minority governments • Government alone cannot pass laws • Role for minority parties • Deals for support
Timing • Select Committee must report back in 6 months (dec 07 + 6/12 = June 08) • Election date?
Timing SC has the options: • Send to the vote advising yes • Send to the vote with changes • Send to the vote advising no • Delay – needs more work
Purpose of the Bill to improve, promote, and protect public health in order to help attain optimal and equitable health outcomes for Maori and all other population groups
The Public Health Bill A law that propose the ways in which normal rights and freedoms can be bypassed to control risks to public health
Fundamental tension The rights of individuals and businesses to go about their affairs free from interference and The rights of individuals and communities to be free from avoidable risks to health
Or – building community Valuing the common good Sanctioning those who betray their fellows Enabling joint action for mutual good
Overview – context 1900 plague in Sydney NZ - 1901 Health Act Population and social changes 1956 Health Act TB Act 1948 Social and technological changes Public Health Bill
Social and technological changes • New and emerging health issues, eg non-communicable conditions, SARS • New strategies to prevent ill-health, eg immunisation and screening • New technologies • Attention to human rights • RMA, Fair Trading Act, HSNO, LGA etc
International obligations • International Health Regulations 1951, 1969 (yellow fever, cholera, plague) • Since then, globalisation, air-travel +++, SARS, avian influenza, radiation, chemical risks • Need to improve (world-wide and in NZ): • emergency management • border health control, • communicable disease management • New IHRs ‘all risks’ in scope
Human Rights The Health Act 1956 shows its age • No attention to privacy issues • No procedural rights eg appeal or review for persons detained • Enhancing human rights can help support public health objectives
Legal context Every sector should do its work safely Workplaces - OSH Health/Hospitals - H&D Services Safety, - HPCAA Roads - Land transport Goods - Fair Trading Regulation under health should be by exception.
New approaches needed • ‘risk-based approach’ • human rights and consultation • international law
PH Bill • Roles • Information • Non-communicable diseases • Conditions posing health risks • TAs • Regulated activities • Emergencies and border health • Miscellaneous
Maori references – purpose (s 3) to improve, promote, and protect public health in order to help attain optimal and equitable health outcomes for Maori and all other population groups …aim to reduce health inequalities by improving health outcomes for Maori and other population groups
Maori references - NCDs (s 80) … the Director-General must take into account the importance of--- … (d) the well-being and mutual interdependence of families and their communities, including whanau, hapu, and iwi: (g) Working towards social and cultural environments conducing to health and well being
Maori references – consultation re individuals (s 110, 131) If a medical officer of health is considering applying to the Court • the medical officer of health may, at his or her discretion, consult with the individual's family or whanau • Can an order be avoided by assistance on the part of the family or whanau;
Maori references – powers of entry and search Marae treated as private dwellings (s 255, 270, 306, 327) (s353) (1) Every entry and search power authorises the person exercising it--- (b) to request any person to assist with the entry and search (including, without limitation, a member of a hapu or iwi if the place to be entered is of cultural or spiritual significance to that hapu or iwi)
Improving health outcomes for Maori? • Tiriti references? • Consultation as in LGA and PHDA? • Principled action to prioritise health of those most affected • What other things can be put into the law to improve health and increase health equity for Maori?
Equity - purpose (s3) Statement of purpose • optimal and equitable health outcomes for Maori and all other population groups • aiming to reduce health inequalities by improving health outcomes for Maori and other population groups
Equity – principles NCDs (s80) take into account • the health of communities • broad determinants of health • involving communities • consultation • mutual interdependence of families and communities, • health status of general population and communities: • social and cultural environments
Equity – objectives (s 47) Cervical screening programme The objectives of the NCSP are to--- inform women and the community of the risks, benefits, and expected population health gains from participation in the NCSP
Equity – definitions • (s4)public health …health of all of the people of New Zealand; or a community or section of those people • (s4) health impact assessment … assess… health of a population or part of a population and the distribution • (s79) risk factor ... incidence of non-communicable diseases in the general population or in communities or in sections of the general population or communities
Equity – questions • Who will be most affected? • Who will benefit the most? • What other things can be put into the law to increase health equity? • What is the evidence (references, please) that changing environments improves equity?
PH functions of DHBs • Employ MOsH and HPOs • Monitor risks to public health • Assess (and report to the DG) those risks • Take steps to contain and manage those risks (where appropriate) (can arrange for another to do)
PH functions of DHBs Lost opportunity to use WHO approach to the essential functions of public health
Essential PH functions according to WHO WPRO Health situation monitoring and analysis Epidemiological surveillance/disease prevention and control Regulation and enforcement to protect public health
Essential PH functionsaccording to WHO WPRO – ctd Health promotion, social participation and empowerment Development of policies and planning in public health Human resources development and planning in public health
Essential PH functions according to WHO WPRO- ctd Research, development and implementation of innovative public health solutions Ensuring the quality of personal and population-based health services Strategic management of health systems and services for population health gain
Information Part 2 Grab-bag of Subsidy compliance verification Cervical screening programme Notification Anonymous hospital data collection (now includes private hospitals) Disclosure to authorised authorities Blood collection(????) Retention of records
Information Part 2 No principles DG annual report on the state of the public health elsewhere DHBs may require a report on risks to health from TAs – but can be charged for it
Information Part 2 This is a lost opportunity to align • DHB obligation to do 3 yearly health needs assessment • TA obligation to survey the district for serious risks to health • TA obligation to 3 yearly report community outcomes
Privacy and individual rights Individual responsibility Community right to protection Political correctness vs vs Conditions posing health risks
Notification (part 2) a more flexible framework • Case, condition, cluster or contaminant (s31) • Medical practitioner + labs+ others +/- vets (s 33-36) • Option for “temporary” status (s38) • “quarantinable “ becomes “epidemic”
Conditions posing health risks Protects public health more • Allows examination on suspicion (s97) • Can have urgent orders (s106) • Offense to recklessly spread (s126)
Conditions posing health risks New provisions for contact tracing • Authorises contact tracing where it doesn’t happen voluntarily (s138-149) • Medical practitioner / MOH may approach employers etc for contact details (s145) • Medical practitioner / MOH may disclose information on risks posed to them to sexual partners / household members (s 150-152)
Conditions posing health risks Respects individual more (s92-93) • Gives a wide range of disease containment options (s95) • Requires use of least restrictive option (s91) • Strengthened safeguards • eg appeals (s112-123), time restrictions (s 96)
Your views How should the balance between individual rights and community protection be reflected in law? How do we defend the rights of communities to be safe when there are those who trivialise the risks by saying that we are too politically correct? What else should be included?
Balancing individual choice with supportive environments - the dreaded Nanny State or sensible controls? Non-communicable diseases
Commercial pressures Individual choice Supportive environments The nanny state vs vs Non-communicable diseases
Non-communicable diseases As proposed by Health Select Committee report on the inquiry into Obesity and Type II Diabetes
Non-communicable diseases Non-binding codes and guidelines (s81-87) Incentive = awards Parliamentary report back • within 3 years, can be extended Can make regulations (s 374 x)