Download
1 / 18
240 likes | 859 Views
Abdominal Aortic Aneurysms. Omaida C. Velazquez, M.D., F.A.C.S. AAA Prevalence. Most AAA's are Never Detected. Approximately 70% to 80% of AAA Patients are Asymptomatic at Initial Diagnosis

E N D
Abdominal Aortic Aneurysms Omaida C. Velazquez, M.D., F.A.C.S
AAA Prevalence • Most AAA's are Never Detected. • Approximately 70% to 80% of AAA Patients are Asymptomatic at Initial Diagnosis • AAA's are Generally Discovered Inadvertently during Procedures to Diagnose Unrelated Medical Conditions • Nearly 200,000 people in the U.S. are diagnosed with AAA annually • Approximately 15,000 Die Each Year from a Ruptured AAA • 45,000 - 50,000 Patients Undergo Surgery • AAA's are More Prevalent in People Over the Age of 60 • More Common in Men than in Women
AAA Symptoms • A pulsing feeling in the abdomen,similar to a heartbeat • Severe, sudden pain in the abdomen or lower back. (aneurysm may be about to rupture) • On rare occasions, feet may develop pain, discoloration, or soreness because of material shed from the aneurysm
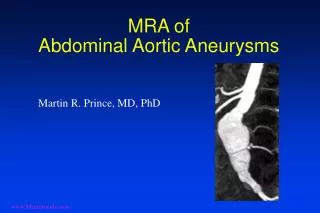
AAA Screening Tests • Abdominal aortic aneurysms are most often found when a physician is performing an imaging test, such as an ultrasound, Hip X-RAY, CT scan, or MRI, for other conditions. • Recommend tests: • Abdominal ultrasound • Computed Tomography (CT) Scan • Magnetic Resonance Imaging (MRI)
The Screening Abdominal Aortic Aneurysms Very Efficiently Act (SAAVE) - 2007 • Important topic right now beginning in January 2007 Medicare will offer • One-time free AAA ultrasound screening to qualified seniors as part of their Welcome to Medicare physical. • Men who have smoked at any time during their life • Men and women with a family history of AAA are eligible for the new Medicare benefit.
How to Proceed After Diagnosis of AAA • Vascular Consultation • Patient Education • Observation with serial Ultrasounds when less than 5 cm in diameter, when asymptomatic • EVAR Vs. Open Repair
Growth Rate Four hundred ninety-two patients were entered into the study with AAAs smaller than 5 cm when first seen. Brown PM, Pattenden R, Vernooy C, Zelt DT, Gutelius JR. Selective management of abdominal aortic aneurysms in a prospective measurement program. J Vasc Surg 1996;23:213-220.
UK Small Aneurysm Trial4.0-5.4 cm Randomized Surgery or Surveillance 1276 Patients Eligible 186 DeclinedRandomization 1090 Underwent Randomization(1991 – 1995) 527 Assigned toUltrasonographic Surveillance 563 Assigned toEarly Elective Surgery 200 Did NotUndergo Surgeryby June 1998 43 Did NotUndergo Surgeryby June 1998 327 Underwent Surgery byJune 1998289 According to Protocol38 In Violation of Protocol 80 Diedby June1998 120 Survivingas ofJune 1998 23 Diedby June1998 20 Survivingas ofJune 1998 520 UnderwentSurgery byJune 1998 62 Underwent Surgery by August 2001 48 Open 13 Endovascular 1 Laparoscopic 33 SurvivingwithoutSurgery as ofAugust 2001 6 SurvivingwithoutSurgery as ofAugust 2001 6 Underwent Surgery by August 2001 5 Open 1 Laparoscopic Only 39 pts. (3.5%) Survived without Surgery - “All Roads Lead to Rome”
Morbidity • 30 day post-op complications after elective AAA repair: • MI 2%-8% • All pulmonary 8%-12% • Reduced renal function 5%-12% • Dialysis 1%-6% • 70% 5 year survival for elective AAA repair Taylor Ann Vasc Surg 1986; 1: 502
Functional Outcomes • 11% transferred to S.N.F 3.66m + 2.9m • All patients were ambulatory pre-op • At median follow up of 25 months • 22% of patients required assistance • 14% were non-ambulatory • 33% of patients reported a decrease in functional status • 18% reported that they would not undergo a repair knowing the recovery process in spite of the risks. W. Kent Williamson, MD et al. Functional outcome after open repair of abdominal aortic aneurysm J Vasc Surg: May 2001 33 • Number 5 • p913 to p920
Open vs. EVAR (Endovascular AAA Repair) Juxtarenal or suprarenal aortic aneurysms, likely need Open Repair
Most Infrarenal Abdominal Aortic Aneurysms (AAA) May be treated by EVAR Glass Model Shows Zenith Stent-graft (COOK)
Endovascular AAA Repair (EVAR)Illustrations Show Powerlink Stent-graft (Endologix)
Open Surgical Repair Longer Recovery Time Longer Hospital Stay 90% Long Term Success Younger patients typically EVAR Shorter length of stay Reduction in blood loss Reduction in OR Time ICU utilization reduced Reduced 30 d morbidity/mortality Older patients typically Needs long-term follow-up May need secondary procedures for endoleaks Open vs. EVAR
“Paradox of Success” Successful Exclusion Anatomy Changes Limb Disconnections Migration Late Failure 1 month and/or 12 month 24 month Parra et al. Journal of Vascular Surgery Vol. 37, No. 1:109
Distribution of Stent Graft Fatigue by Device *Excluding patient with acute conversion †Excluding those patients who underwent open conversion and stent graft explanation ‡Including emergent use not part of clinical study Jacobs TS, Won J, Graveraux EC, Faries PL, Morrissey N, Teodorescu VJ, et al. Mechanical failure of prosthetic human implants: a ten-year experience with aortic stent graft devices. J Vasc Surg 2003;37:16-21.
100% Endo-Exuberance 75% Aggressive 60% Increasing Use of EVAR as aPercentage of All AAA Repairs Endo-Realism Average 40% Conservative 25% Endo-Apathy Viable Technology Institutions performing far greater than 75% of all AAA repairs with EVAR may be experiencing “Endo-Exuberance,” while those with less than a 25% utilization may be suffering from “Endo-Apathy.” w. Charles Sternbergh, III, et Endo-Exuberance to Endo-Reality: Trends in the Management of 431 AAA Repairs Between 1996 and 2002. Journal of Endovascular Therapy: Vol. 10, No. 3, pp. 418-423.