Download
1 / 32
330 likes | 913 Views
Aortic Dissection and Aneurysms. Presented by Dr. Daniel Kranitz Prepared by Mary Edwards September 27, 2005 Tintanalli Chapter 58, Pages 404-409. Abdominal Aortic Aneurysms (AAA). Risk factors Elderly (>60) Familial trend (18% with 1 ° relative) Connective Tissue D/O (Marfan’s)

E N D
Aortic Dissection and Aneurysms Presented by Dr. Daniel Kranitz Prepared by Mary Edwards September 27, 2005 Tintanalli Chapter 58, Pages 404-409
Abdominal Aortic Aneurysms (AAA) • Risk factors • Elderly (>60) • Familial trend (18% with 1° relative) • Connective Tissue D/O (Marfan’s) • Other aneurysms • Atherosclerosis (HTN, Lipids, smoking, DM)
AAA • Pathogenesis • Intima infiltrated by atherosclerosis and thinned media. • Possible intraluminal thrombus and adventitia infiltrated by inflammatory cells
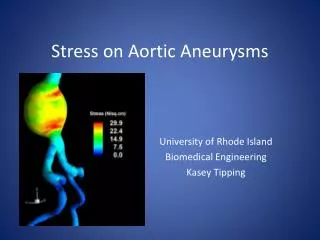
AAA • Average rate of growth 0.25-0.5 cm per year. • Larger aneurysms extend more rapidly than smaller ones. (LaPlace law)
AAA • Clinical Features • Syncope (10-12%) • Back and/or Abdominal Pain –severe and abrupt, ripping or tearing sensation (50%) • Shock –intraperitoneal rupture, massive blood loss • Sudden death
AAA • Physical Exam • Pain on palpation or not • Retroperitoneal hematoma • Cullen sign (periumbilical ecchymosis) • Grey-Turner sign (flank ecchymosis) • Scrotal hematoma or inguinal mass (blood dissecting to these areas) • Iliopsoas sign • Femoral nerve neuropathy
AAA • Found aneurysms refer to follow up • >5cm diameter –increased chance of rupture • <5cm –decreased chance of rupture • Symptomatic aneurysms of any size = Emergency!!
AAA • Diagnosis • Includes differential diagnoses of syncope, abd pain, CP, back pain and shock. • If with combo of two or more think aortic dz.
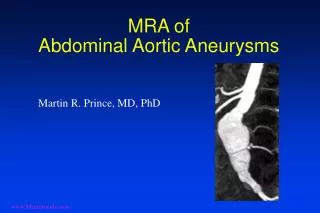
AAA • Radiologic Evaluation • Should not delay operative treatment!! • Plain abd film (calcified bulging) • US (bedside, up to 100% sensitive, not reliable to detect rupture) • CT (with IV contrast only if stable) • MRI
AAA • ED Treatment • Urgent surgical consult • Make diagnosis & assist rapid transfer to OR • 2 large bore IVs • Cardiac Monitor • O2 • ? Blood transfusion • IV fluid resuscitation –controversial amount b/c too much can be harmful • RADIOGRAPHIC STUDIES ONLY IF UNLIKELY TO HAVE RUPTURED AAA!!!
AAA • ½ of patients with ruptured AAA who reach the OR die!
A Bit About Thoracic Aortic Aneursym • Presenting symptoms include esophageal, tracheal, bronchial, or even neurologic disorders. • If it erodes to adjacent structures it is immediately fatal!!
Aortic Dissection • Pathogenesis • Prominent cause of sudden death • Presents with severe abd., chest, and back pain • Violation of intima that allows blood to enter media and dissect b/w intimal and adventitial layers • Common site is ascending aorta at ligamentum arteriosum
Aortic Dissection • Common presenting groups • >50 yoa with HTN • 2/3 male • Marfan’s syndrome • Congenital heart disease • Pregnancy
Aortic Dissection • Stanford Classification • Type A -involves ascending aorta • Type B –involves descending aorta • DeBakey Classification • Type I –ascending, arch & descending aorta • Type II –ascending only • Type III –descending only
Aortic Dissection • Clinical Features • >85% abrupt, severe pain in chest or b/w scapula • 50% ripping or tearing • Pain in anterior chest –ascending aorta (70%) • Back pain (less common) –descending aorta (63%) • If dissection into carotid classic neuro symptoms
Aortic Dissection • Clinical Features • 40% with neurologic sequelae (ex. paraplegia) • Nausea, vomiting, diaphoresis • Most have sense of impending doom!
Aortic Dissection • Physical Exam • Usually normal heart and lung exam • May have aortic insufficiency • <20% with decreased radial, femoral or carotid pulse • HTN • Tachycardia • Hypotension
Aortic Dissection • Physical Exam • Pericardial tamponade (muffled heart tones, JVD, pulsus paradoxus) • Hoarseness (compression of recurrent laryngeal nerve) • Horner’s Syndrome (compression of superior cervical sympathetic ganglion)
Aortic Dissection • Diagnosis • Ischemic end-organ manifestation such as MI, pericardial dz, pulmonary d/o, stroke, SCI, musculoskeletal dz of extremities, intraabdominal ischemia. • Can change location with time as dissects.
Aortic Dissection • Thoracic Dissection • 90% have abnormal CXR • Widened mediastinum • Abnormal aortic contour • Pleural effusion • Deviation of trachea, mainstem bronchi, or esophagus • Intimal calcium visable & distant from edge (calcium sign)
Aortic Dissection • Diagnosis • CT • 83-100% sensitive • 87-100% specific • Use spiral CT with IV contrast • Will not give anatomic details of arterial branches or aortic valve competence. • Modality of choice in unstable patient
Aortic Dissection • Diagnosis • Angiography • “Gold standard” • Shows all anatomy and involvement • 94% specific • 88% sensitive • TEE • 97-100% sensitive • 97-99% specific • Esophageal dz contraindication
Aortic Dissection • In contrast to ruptured AAA, SUSPECTED DISSECTIONS MUST BE CONFIRMED RADIOLOGICALLY PRIOR TO SENDING TO OR!!!
Aortic Dissection • ED Treatment • Treat hypertension • -blocker • Esmolol 500g/kg IV bolus over 1 minute then 50-150 g/kg minute • Metoprolol 5mg q2min x3 IV then 2-5mg/hr • Propranolol 20mg IV then 40mg, 8-mg q10min to 300mg total • Calcium channel blocker if -blocker contraindicated
Aortic Dissection • ED Treatment • Vasodilator • Nitroprusside 0.3 g/kg/min IV • Surgery • OR for ascending aortic dissection • Descending aortic dissection worse surgical risks –controversial for repair
Questions • 1. A patient with a suspected aortic dissection should be immediately tranferred to OR without radiographic studies. • A. True • B. False
2. Females are more likely than males to develop aortic dissection. • A. True • B. False • 3. Dissection of the ascending aorta only is DeBakey classification • A. Type I • B. Type II • C. Type III • D. Type A • E. Type B
4. Patients with a ruptured AAA can present with all of the following symptoms except • A. Shock • B. Syncope • C. Sudden death • D. Nausea and vomiting • E. Headache
5. Which of the following radiologic modalities is considered the “gold standard” for diagnosing an aortic dissection? • A. CT • B. MRI • C. TEE • D. Angiography • E. CXR
Answers • 1. B • 2. B • 3. B • 4. E • 5. D