Download
1 / 15
150 likes | 182 Views
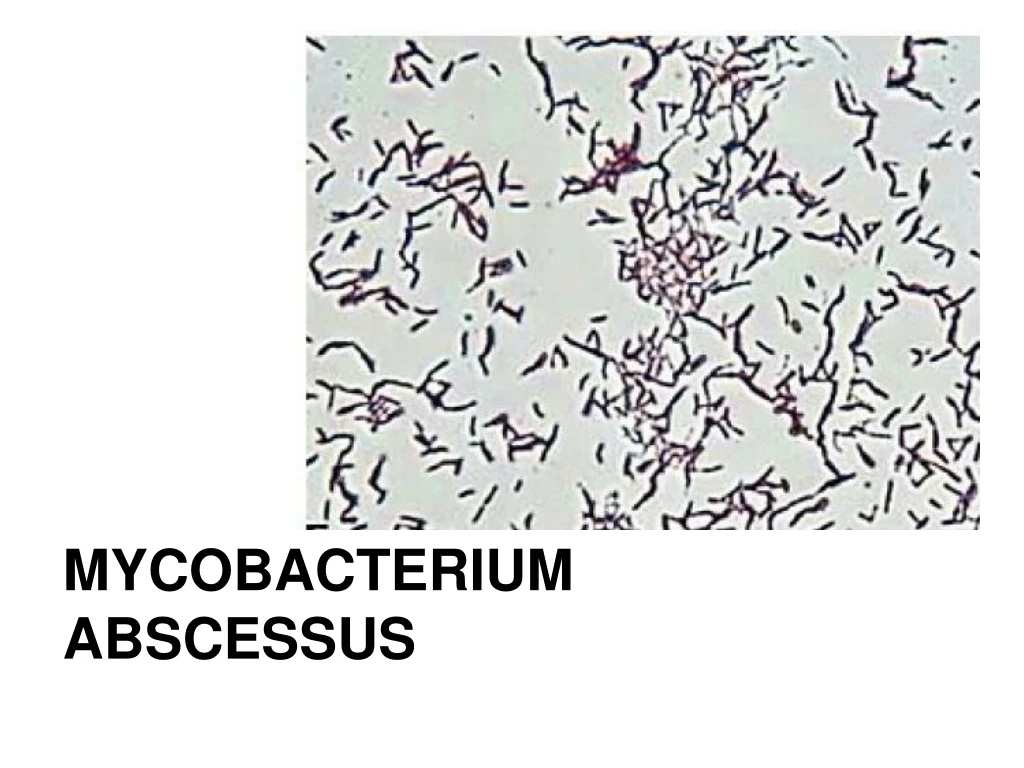
Mycobacterium abscessus, formerly part of M. chelonae-complex, is a chemotherapy-resistant, rapid-growing mycobacterium. It causes pulmonary and cutaneous disease, with rare cases of disseminated disease. Clusters of infections have been reported after cosmetic injections. Treatment strategies include combination therapy with clarithromycin, amikacin, and either cefoxitin or imipenem.

E N D
Mycobacterium abscessus • Rapid growing mycobacterium • Environmental contaminant • Formerly part of “M. chelonae-complex” till 1992 • Subspecies of M. abscessus • M. abscessus senso strictu • M. massiliense • M. bolletii
Mycobacterium abscessus Pulmonary disease most common Cutaneous disease Disseminated disease rare (mostly immunosuppressed w/ corticosteroids) Bacteremia/ endocarditis: described in hemodialysis patients
Clusters of M. abscessus infection after cosmetic Rx or injection of alternative medicine
Mycobacterium abscessus • Most pathogenic and chemotherapy-resistant rapid-growing mycobacterium • Intrinsic resistance • Low permeability of cell wall • Drug export systems • Antibiotic-modifying/ inactivating enzymes • Genetic polymorphism of targeted gene • Acquired resistance • Macrolide resistance • Aminoglycoside resistance
Intrinsic resistance • Low permeability of cell wall • High lipid content (up to 60% of dry weight) • Drug export systems • Mycobacterial membrane protein large (MmpL) transporter family • ABC-type multidrug transporter family
Intrinsic resistance • Antibiotic-modifying/ inactivating enzymes • Rifampicin ADP-ribosyltransferase and mono-oxygenase → rifampicin resistance • Aminoglycoside 2-N-acetyltransferase and phosphotransferases → aminoglycosiade resistance • Genetic polymorphism of target genes • Mutations in embB → ethambutol resistance • Mutations in quinolone resistance-determining regions (QRDRs) → fluoroquinolones resistance
Acquired resistance • Macrolide resistance • Macrolide → inhibit ribosomal translocation • Inducible ribosomal methylase erm(41) gene → modify ribosome binding site • Clarithromycin induces erm(41) to a significantly greater extent than azithromycin • ??azithromycin preferred over clarithromycin
Acquired resistance • Aminoglycoside resistance • Aminoglycoside → interfere proof-reading process, causing errors in synthesis with premature termination • Mutations affecting 16S rRNA
Treatment strategy • Limited, extra-pulmonary disease • Clarithromycin alone (Acquired mutational resistance not observed when treating localized infections with macrolide monotherapy) • Amikacin +/- cefoxitin/ imipenem may be added for two weeks until clinical improvement in more severe cases • Duration guided by clinical response: typically 4 months. Osteomyelitis: 6 month minimum recommended • Infected foreign bodies should be removed
Treatment strategy • Pulmonary or severe extrapulmonary disease • In vitro data not yielded effective regimen for treating pulmonary disease • May not achieve sputum culture negativity even with 12 months of therapy • Lung disease should be considered a chronic, incurable infection
Treatment strategy • Pulmonary or severe extrapulmonary disease • Combination therapy always recommended: • Clarithromycin 500mg PO BD plus Amikacin IV (15mg/kg/d) plus either cefoxitin IV (2gm Q4H) or Imipenem IV (1gm Q6H) • Duration: combination therapy w/ injectable agents + clarithromycin at least 2-4 months but duration often limited by adverse effects • Maintenance: once with good effect with combination therapy, consider switch to oral clarithromycin OR azithromycin indefinitely ("suppressive treatment")
Treatment strategy • Pulmonary or severe extrapulmonary disease • Other agents: little good data to guide on selection or use in combination • Tigecycline 100mg IV load then 50mg IV Q12H • Little reported clinical data but may be in vitro susceptible and could be substituted as one of the injectables. Often poorly tolerated due to GI distress
Treatment strategy • Pulmonary or severe extrapulmonary disease • Linezolid 600mg Q12H PO • potentially useful oral agent in pts in whom parental Rx not tolerated or feasible • Clofazimine • may have in vitro activity, little clinical experience
Mycobacterium abscessus Most pathogenic and chemotherapy-resistant rapid growing mycobacterium Most commonly caused pulmonary disease Clusters of cutaneous disease after cosmetic injections reported Disseminated disease/ bacteremia is rare ?related to severe DIC, but no case report identified