Download

1 / 83
930 likes | 1.39k Views
Mycobacterium leprae. For MBBS (05-12-2017). Disease of Historical importance World's oldest recorded disease Stigmatized disease Gerhard Henrick Armauer Hansen (1873-Norway). The Bacterium. Armauer Hansen in 1868.

E N D
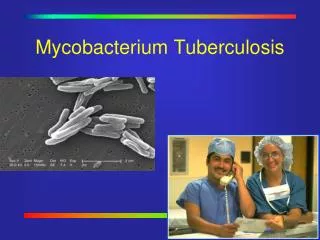
Mycobacterium leprae For MBBS (05-12-2017)
Disease of Historical importance • World's oldest recorded disease • Stigmatized disease • Gerhard HenrickArmauer Hansen (1873-Norway)
Armauer Hansen in 1868 Morphology :Straight rods. 1 - 8 x 0.2 - 0.5µmSingle / groups. Intracellular.Acid fast bacilli with 5% H2 SO4.As agglomerates, bacilli being bound together by a lipid like substance (Glia) – called GLOBI
Parallel rows of bacilli in globi: CIGAR BUNDLE appearance – as in tissue section clumps of bacilli resemble cigarette ends • GLOBI is seen in Virchow’s lepra cell or foamy cells (Large undifferentiated histiocytes)
Cultivation No artificial media / tissue culture available.Generation time: 12-13 daysMouse :Intradermally into Foot pads.Granulomatous lesions in 1- 6 months.Intact CMI : Limited replication.↓CMI : Generalized leprosy.Armadillo:Highly susceptible.Chimpanzees, Mangabey monkey.
Adaptation in artificial media: ICRC, Bombay 1962. – AFB from leprosy patients were isolated in human fetal spinal ganglion cell culture= ICRC bacillus (LJ adapted)
Resistance Warm humid environment 9 - 16 days. 46 days in Moist soil 2 hoursinSunlight 30 minutes U V rays
Epidemiology Exclusively Human disease & only source is a patientExact mode of transmission – not clear; probably via -Nasal secretions.(One nasal blow may release 8 x 108 bacilli)Entry via – respiratory tract or skinAsymptomatic infection not uncommon
Not very communicable – 5% spouses suffer Incubation period is 3-5 years. (2to 40 yrs)Continuous close contact.Rare in children < 5 Years. Confined to underdeveloped tropical countries & southern hemisphere currently India • Prevalence 0.68/10000 population in 2012 • 32 states/UT achieved target of elimination • Chhattisgarh, Dadar & Nagar Haveli Prevalence >1/10000
Annual Report 2015-16 from NLEP GOI (as on 1st April 2016) • >1/10,000 Population (163 District out of 669) • Total cases 86028
Annual Report 2015-16 from NLEP GOI • >1-Chattisgarh, Dadar Nagar Haveli, Delhi, Odisha, Chandigarh, Lakshadeep
IV. WHO classification Based on bacterial load. 1. Paucibacillary I, T T, BT 2. Multibacillary BB, BL, LL.
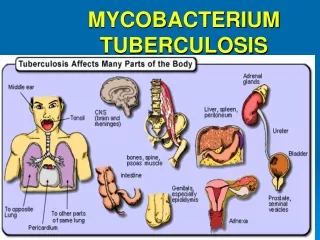
Leprosy Slow, chronic & progressive Granulomatous disease of Peripheral nerves,skin and Muco- cutaneous tissues (Nasal mucosa).It affects Skin, liver, testes ,bones.
Pathogenesis Source : Nasal or Skin discharges from lesion. Portal of entry: Damaged skin -Inoculation.Nasal mucosa- Inhalation
Pathogenesis contd….: Infiltration of bacilli in cooler body tissues like skin (nose, outer ear), testicles & superficial nerve endings→ (maculae) visible lesions. A non-specific or Indeterminate skin lesion is the First sign of disease.Schwann cell is target cell. Neuritis leads to Anesthesia & muscle paralysis.
Lepromatous leprosy • Extensive • maculae, • papules or • nodules; • Extensive • destruction of skin. • CMI severely depressed • High infectivity • Tuberculoid leprosy • Lesions are • large maculae on skin, • superficial nerve • endings. • CMI is intact. • Low infectivity Regression Progression
Lepromatous leprosy Generalized form with decreased CMI. “Lepromata” : Granulation tissue with plenty of vacuolated cells, from MN cells to Lepra cells. Ulceration Secondary infection & Mutilation of limbs.Skin lesions are extensive and bilaterally symmetrical.
Sites: Commonly face, ear lobules, hands and feet. • Symmetrical thickening of peripheral nerves & anesthesia • Bacilli invade mucosa of Nose , Mouth and Respiratory tract → shed in secretions. • Bacteremia present. • RE system, Eyes, testes, kidney & bone involved
Lepromin test is negative. CD8+ cells in plenty • Antibodies / other Abs are seen (exaggerated humoral response) • BFP= syphilis tests (STS) • Infective form….more than other types – poor prognosis • Lateral part of eyebrows are lost
Lepromatous leprosy Lepromatous leprosy
Complications :Acute exacerbations. Testicular atrophy, Gynaecomastia Diffuse thickening of face – (Leonine face). Necrosis of nasal bones, cartilage with loss of upper incisors. Corneal ulcers.
Tuberculoid leprosy Localized form in individuals with intact CMI.Skin lesions :Few hypo or hyper pigmented macular patches (anesthetic)Sharply demarcatedSeen on Face, trunk and limbs.Bacilli are scanty or absent. (paucibacillary)Infectivity is low.
Diagnosed with Clinical + Histological evidences.Nerves : Peripheral Nerves to bigger nerves involved.Thickened, hard and tender.Deformities in hand & feet Lepromin test is positive.Auto antibodies production is rare. CD4+ cells.
Complications Peripheral neuropathy. V & VII th cranial nerve : Corneal ulcers.Ulnar nerve : Claw hand.Lateral popliteal nerve : Foot drop. Posterior tibial & medial nerve: Trophic ulcers, Loss of digits.
Dimorphous/Borderline type : Lesions resembles both LL (bacteriology) & T T (Clinically). May turn to complete LL or T T type (depending on host resistance or chemo therpay)
Borderline lepromatous Borderline tuberculoid leprosy Lesions are Slightly asymmetrical with or without anesthesia. Cirular, sharply demarcated lesions. Raised erythematous border with anesthesia.
Indeterminate type: Early stages : Maculoanesthetic patches. Lesions are not like T T or LL Spontaneous healing. Turn to either LL or T T type.
Immunity :High degree of innate immunity. Induces both AMI & CMI. Antibodies are not effective. LL Pts : Large number of CD8 cells. TT Pts : Predominantly CD4 cells.Genetic relation: T T : HLA – DR2 L L : HLA MTI, DQ1
Differential diagnosis of Leprosy Birth mark T. versicolor T.corporis
Pytiriasis alba Vitiligo Lichen planus