Download
1 / 1
10 likes | 116 Views
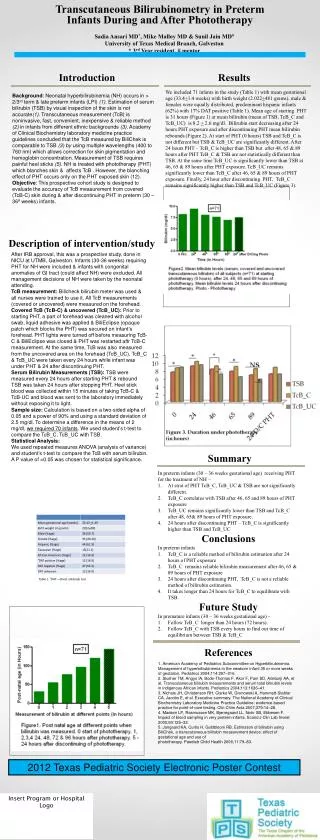
From abnormal chest X-ray to a rare cardiac anomaly. Unnati Doshi MD, MPH, (PGY 5), William Carson MD, Larry Kramer, MD, Duraisamy Balaguru MD Department of Pediatric Cardiology University of Texas Medical School at Houston. Abstract. Innominate Vein.

E N D
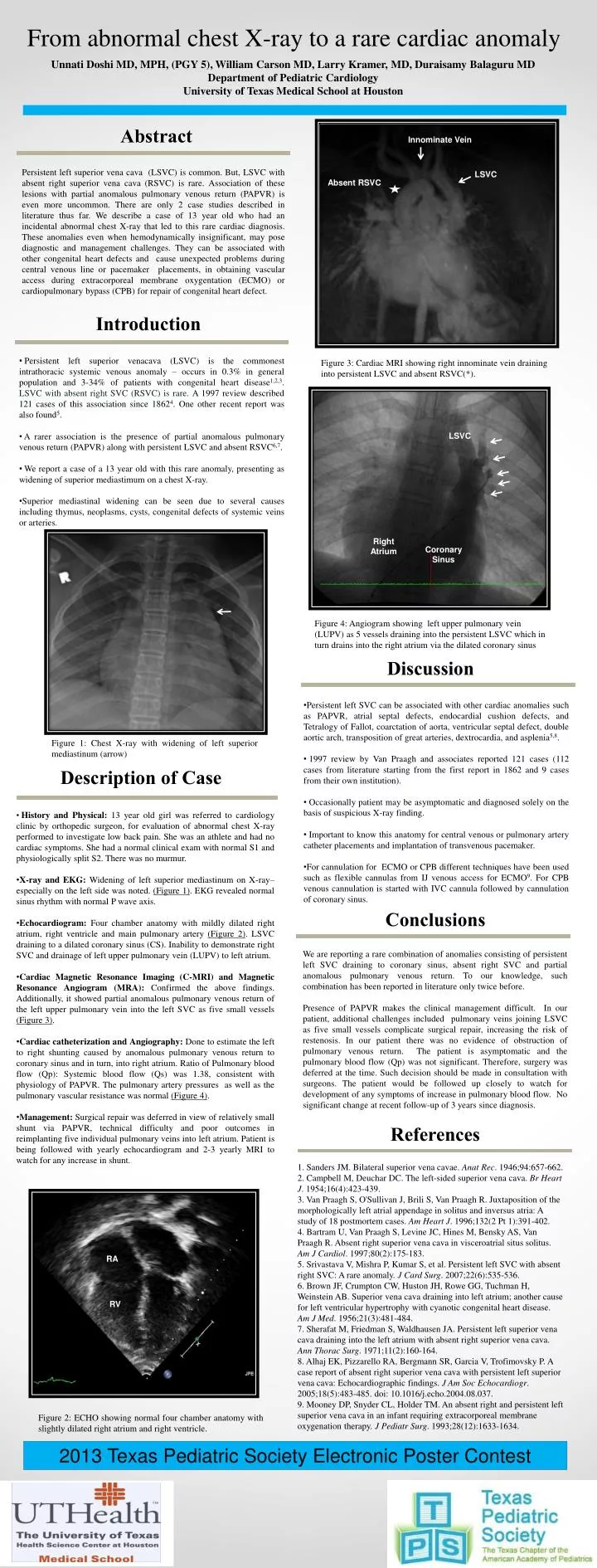
From abnormal chest X-ray to a rare cardiac anomaly Unnati Doshi MD, MPH, (PGY 5), William Carson MD, Larry Kramer, MD, Duraisamy Balaguru MD Department of Pediatric Cardiology University of Texas Medical School at Houston Abstract Innominate Vein Persistent left superior vena cava (LSVC) is common. But, LSVC with absent right superior vena cava (RSVC) is rare. Association of these lesions with partial anomalous pulmonary venous return (PAPVR) is even more uncommon. There are only 2 case studies described in literature thus far. We describe a case of 13 year old who had an incidental abnormal chest X-ray that led to this rare cardiac diagnosis. These anomalies even when hemodynamically insignificant, may pose diagnostic and management challenges. They can be associated with other congenital heart defects and cause unexpected problems during central venous line or pacemaker placements, in obtaining vascular access during extracorporeal membrane oxygentation (ECMO) or cardiopulmonary bypass (CPB) for repair of congenital heart defect. LSVC Absent RSVC Introduction • Persistent left superior venacava (LSVC) is the commonest intrathoracic systemic venous anomaly – occurs in 0.3% in general population and 3-34% of patients with congenital heart disease1,2,3. LSVC with absent right SVC (RSVC) is rare. A 1997 review described 121 cases of this association since 18624. One other recent report was also found5. • A rarer association is the presence of partial anomalous pulmonary venous return (PAPVR) along with persistent LSVC and absent RSVC6,7. • We report a case of a 13 year old with this rare anomaly, presenting as widening of superior mediastimum on a chest X-ray. • Superior mediastinal widening can be seen due to several causes including thymus, neoplasms, cysts, congenital defects of systemic veins or arteries. Figure 3: Cardiac MRI showing right innominate vein draining into persistent LSVC and absent RSVC(*). LSVC Right Atrium Coronary Sinus Figure 4: Angiogram showing left upper pulmonary vein (LUPV) as 5 vessels draining into the persistent LSVC which in turn drains into the right atrium via the dilated coronary sinus Discussion • Persistent left SVC can be associated with other cardiac anomalies such as PAPVR, atrial septal defects, endocardial cushion defects, and Tetralogy of Fallot, coarctation of aorta, ventricular septal defect, double aortic arch, transposition of great arteries, dextrocardia, and asplenia5,8. • 1997 review by Van Praagh and associates reported 121 cases (112 cases from literature starting from the first report in 1862 and 9 cases from their own institution). • Occasionally patient may be asymptomatic and diagnosed solely on the basis of suspicious X-ray finding. • Important to know this anatomy for central venous or pulmonary artery catheter placements and implantation of transvenous pacemaker. • For cannulation for ECMO or CPB different techniques have been used such as flexible cannulas from IJ venous access for ECMO9. For CPB venous cannulation is started with IVC cannula followed by cannulation of coronary sinus. Figure 1: Chest X-ray with widening of left superior mediastinum (arrow) Description of Case • History and Physical: 13 year old girl was referred to cardiology clinic by orthopedic surgeon, for evaluation of abnormal chest X-ray performed to investigate low back pain. She was an athlete and had no cardiac symptoms. She had a normal clinical exam with normal S1 and physiologically split S2. There was no murmur. • X-ray and EKG: Widening of left superior mediastinum on X-ray– especially on the left side was noted. (Figure 1). EKG revealed normal sinus rhythm with normal P wave axis. • Echocardiogram: Four chamber anatomy with mildly dilated right atrium, right ventricle and main pulmonary artery (Figure 2). LSVC draining to a dilated coronary sinus (CS). Inability to demonstrate right SVC and drainage of left upper pulmonary vein (LUPV) to left atrium. • Cardiac Magnetic Resonance Imaging (C-MRI) and Magnetic Resonance Angiogram (MRA): Confirmed the above findings. Additionally, it showed partial anomalous pulmonary venous return of the left upper pulmonary vein into the left SVC as five small vessels (Figure 3). • Cardiac catheterization and Angiography: Done to estimate the left to right shunting caused by anomalous pulmonary venous return to coronary sinus and in turn, into right atrium. Ratio of Pulmonary blood flow (Qp): Systemic blood flow (Qs) was 1.38, consistent with physiology of PAPVR. The pulmonary artery pressures as well as the pulmonary vascular resistance was normal (Figure 4). • Management: Surgical repair was deferred in view of relatively small shunt via PAPVR, technical difficulty and poor outcomes in reimplanting five individual pulmonary veins into left atrium. Patient is being followed with yearly echocardiogram and 2-3 yearly MRI to watch for any increase in shunt. Conclusions We are reporting a rare combination of anomalies consisting of persistent left SVC draining to coronary sinus, absent right SVC and partial anomalous pulmonary venous return. To our knowledge, such combination has been reported in literature only twice before. Presence of PAPVR makes the clinical management difficult. In our patient, additional challenges included pulmonary veins joining LSVC as five small vessels complicate surgical repair, increasing the risk of restenosis. In our patient there was no evidence of obstruction of pulmonary venous return. The patient is asymptomatic and the pulmonary blood flow (Qp) was not significant. Therefore, surgery was deferred at the time. Such decision should be made in consultation with surgeons. The patient would be followed up closely to watch for development of any symptoms of increase in pulmonary blood flow. No significant change at recent follow-up of 3 years since diagnosis. References 1. Sanders JM. Bilateral superior vena cavae. Anat Rec. 1946;94:657-662. 2. Campbell M, Deuchar DC. The left-sided superior vena cava. Br Heart J. 1954;16(4):423-439. 3. Van Praagh S, O'Sullivan J, Brili S, Van Praagh R. Juxtaposition of the morphologically left atrial appendage in solitus and inversus atria: A study of 18 postmortem cases. Am Heart J. 1996;132(2 Pt 1):391-402. 4. Bartram U, Van Praagh S, Levine JC, Hines M, Bensky AS, Van Praagh R. Absent right superior vena cava in visceroatrial situs solitus. Am J Cardiol. 1997;80(2):175-183. 5. Srivastava V, Mishra P, Kumar S, et al. Persistent left SVC with absent right SVC: A rare anomaly. J Card Surg. 2007;22(6):535-536. 6. Brown JF, Crumpton CW, Huston JH, Rowe GG, Tuchman H, Weinstein AB. Superior vena cava draining into left atrium; another cause for left ventricular hypertrophy with cyanotic congenital heart disease. Am J Med. 1956;21(3):481-484. 7. Sherafat M, Friedman S, Waldhausen JA. Persistent left superior vena cava draining into the left atrium with absent right superior vena cava. Ann Thorac Surg. 1971;11(2):160-164. 8. Alhaj EK, Pizzarello RA, Bergmann SR, Garcia V, Trofimovsky P. A case report of absent right superior vena cava with persistent left superior vena cava: Echocardiographic findings. J Am Soc Echocardiogr. 2005;18(5):483-485. doi: 10.1016/j.echo.2004.08.037. 9. Mooney DP, Snyder CL, Holder TM. An absent right and persistent left superior vena cava in an infant requiring extracorporeal membrane oxygenation therapy. J Pediatr Surg. 1993;28(12):1633-1634. RA RV Figure 2: ECHO showing normal four chamber anatomy with slightly dilated right atrium and right ventricle. 2013 Texas Pediatric Society Electronic Poster Contest Insert Program for Hospital Logo


![[Insert Hospital Name]](https://cdn0.slideserve.com/59021/insert-hospital-name-dt.jpg)

![[Insert Client Logo]](https://cdn1.slideserve.com/1968686/slide1-dt.jpg)

![[Insert Client Logo]](https://cdn1.slideserve.com/2208608/slide1-dt.jpg)