Download
1 / 1

E N D
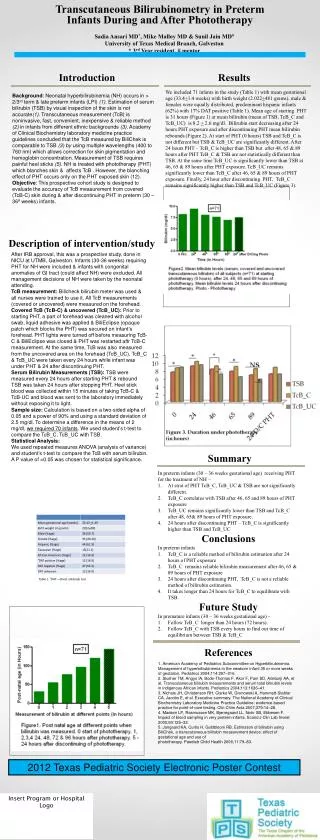
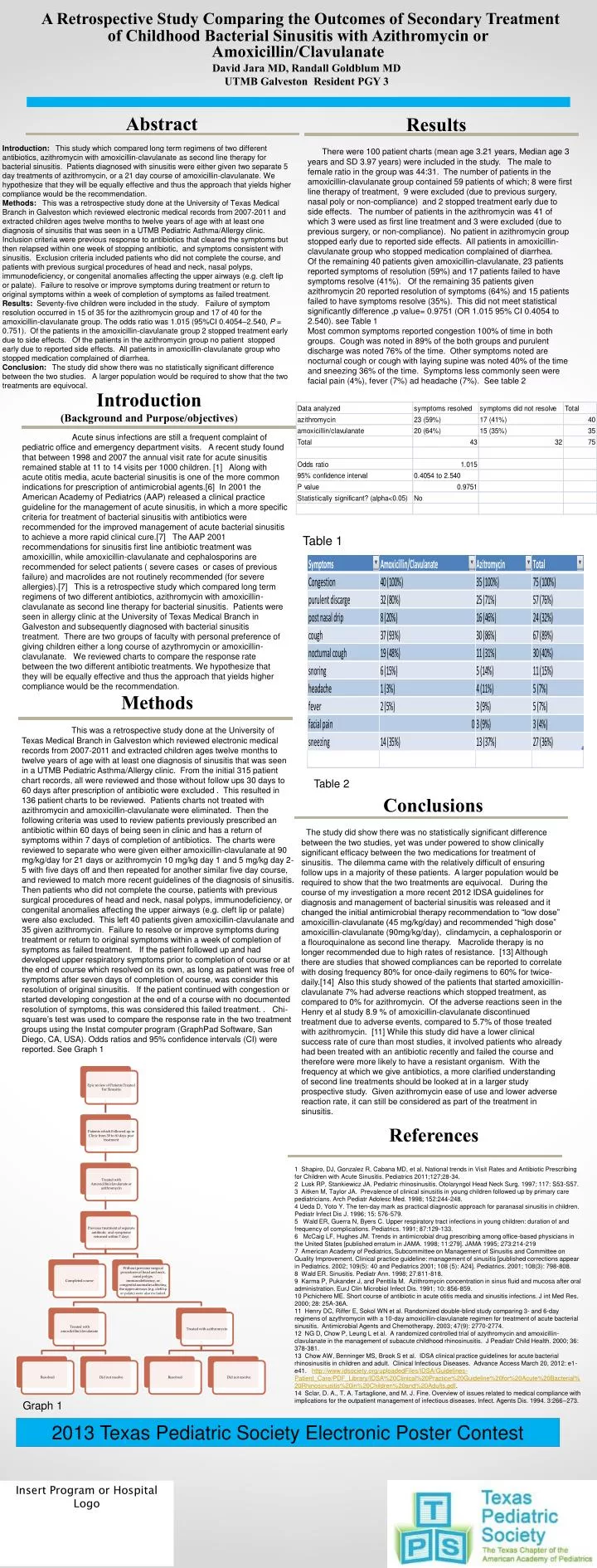
This was a retrospective study done at the University of Texas Medical Branch in Galveston which reviewed electronic medical records from 2007-2011 and extracted children ages twelve months to twelve years of age with at least one diagnosis of sinusitis that was seen in a UTMB Pediatric Asthma/Allergy clinic. From the initial 315 patient chart records, all were reviewed and those without follow ups 30 days to 60 days after prescription of antibiotic were excluded . This resulted in 136 patient charts to be reviewed. Patients charts not treated with azithromycin and amoxicillin-clavulanate were eliminated. Then the following criteria was used to review patients previously prescribed an antibiotic within 60 days of being seen in clinic and has a return of symptoms within 7 days of completion of antibiotics. The charts were reviewed to separate who were given either amoxicillin-clavulanate at 90 mg/kg/day for 21 days or azithromycin 10 mg/kg day 1 and 5 mg/kg day 2-5 with five days off and then repeated for another similar five day course, and reviewed to match more recent guidelines of the diagnosis of sinusitis. Then patients who did not complete the course, patients with previous surgical procedures of head and neck, nasal polyps, immunodeficiency, or congenital anomalies affecting the upper airways (e.g. cleft lip or palate) were also excluded. This left 40 patients given amoxicillin-clavulanate and 35 given azithromycin. Failure to resolve or improve symptoms during treatment or return to original symptoms within a week of completion of symptoms as failed treatment. If the patient followed up and had developed upper respiratory symptoms prior to completion of course or at the end of course which resolved on its own, as long as patient was free of symptoms after seven days of completion of course, was consider this resolution of original sinusitis. If the patient continued with congestion or started developing congestion at the end of a course with no documented resolution of symptoms, this was considered this failed treatment. . Chi-square’s test was used to compare the response rate in the two treatment groups using the Instat computer program (GraphPad Software, San Diego, CA, USA). Odds ratios and 95% confidence intervals (CI) were reported. See Graph 1 A Retrospective Study Comparing the Outcomes of Secondary Treatment of Childhood Bacterial Sinusitis with Azithromycin or Amoxicillin/Clavulanate David Jara MD, Randall Goldblum MD UTMB Galveston Resident PGY 3 Abstract Results Introduction: This study which compared long term regimens of two different antibiotics, azithromycin with amoxicillin-clavulanate as second line therapy for bacterial sinusitis. Patients diagnosed with sinusitis were either given two separate 5 day treatments of azithromycin, or a 21 day course of amoxicillin-clavulanate. We hypothesize that they will be equally effective and thus the approach that yields higher compliance would be the recommendation. Methods: This was a retrospective study done at the University of Texas Medical Branch in Galveston which reviewed electronic medical records from 2007-2011 and extracted children ages twelve months to twelve years of age with at least one diagnosis of sinusitis that was seen in a UTMB Pediatric Asthma/Allergy clinic. Inclusion criteria were previous response to antibiotics that cleared the symptoms but then relapsed within one week of stopping antibiotic, and symptoms consistent with sinusitis. Exclusion criteria included patients who did not complete the course, and patients with previous surgical procedures of head and neck, nasal polyps, immunodeficiency, or congenital anomalies affecting the upper airways (e.g. cleft lip or palate). Failure to resolve or improve symptoms during treatment or return to original symptoms within a week of completion of symptoms as failed treatment. Results: Seventy-five children were included in the study. Failure of symptom resolution occurred in 15 of 35 for the azithromycin group and 17 of 40 for the amoxicillin-clavulanate group. The odds ratio was 1.015 (95%CI 0.4054–2.540, P = 0.751). Of the patients in the amoxicillin-clavulanate group 2 stopped treatment early due to side effects. Of the patients in the azithromycin group no patient stopped early due to reported side effects. All patients in amoxicillin-clavulanate group who stopped medication complained of diarrhea. Conclusion: The study did show there was no statistically significant difference between the two studies. A larger population would be required to show that the two treatments are equivocal. There were 100 patient charts (mean age 3.21 years, Median age 3 years and SD 3.97 years) were included in the study. The male to female ratio in the group was 44:31. The number of patients in the amoxicillin-clavulanate group contained 59 patients of which; 8 were first line therapy of treatment, 9 were excluded (due to previous surgery, nasal poly or non-compliance) and 2 stopped treatment early due to side effects. The number of patients in the azithromycin was 41 of which 3 were used as first line treatment and 3 were excluded (due to previous surgery, or non-compliance). No patient in azithromycin group stopped early due to reported side effects. All patients in amoxicillin-clavulanate group who stopped medication complained of diarrhea. Of the remaining 40 patients given amoxicillin-clavulanate, 23 patients reported symptoms of resolution (59%) and 17 patients failed to have symptoms resolve (41%). Of the remaining 35 patients given azithromycin 20 reported resolution of symptoms (64%) and 15 patients failed to have symptoms resolve (35%). This did not meet statistical significantly difference ,p value= 0.9751 (OR 1.015 95% CI 0.4054 to 2.540). see Table 1 Most common symptoms reported congestion 100% of time in both groups. Cough was noted in 89% of the both groups and purulent discharge was noted 76% of the time. Other symptoms noted are nocturnal cough or cough with laying supine was noted 40% of the time and sneezing 36% of the time. Symptoms less commonly seen were facial pain (4%), fever (7%) ad headache (7%). See table 2 Introduction (Background and Purpose/objectives) Acute sinus infections are still a frequent complaint of pediatric office and emergency department visits. A recent study found that between 1998 and 2007 the annual visit rate for acute sinusitis remained stable at 11 to 14 visits per 1000 children. [1] Along with acute otitis media, acute bacterial sinusitis is one of the more common indications for prescription of antimicrobial agents.[6] In 2001 the American Academy of Pediatrics (AAP) released a clinical practice guideline for the management of acute sinusitis, in which a more specific criteria for treatment of bacterial sinusitis with antibiotics were recommended for the improved management of acute bacterial sinusitis to achieve a more rapid clinical cure.[7] The AAP 2001 recommendations for sinusitis first line antibiotic treatment was amoxicillin, while amoxicillin-clavulanate and cephalosporins are recommended for select patients ( severe cases or cases of previous failure) and macrolides are not routinely recommended (for severe allergies).[7] This is a retrospective study which compared long term regimens of two different antibiotics, azithromycin with amoxicillin-clavulanate as second line therapy for bacterial sinusitis. Patients were seen in allergy clinic at the University of Texas Medical Branch in Galveston and subsequently diagnosed with bacterial sinusitis treatment. There are two groups of faculty with personal preference of giving children either a long course of azythromycin or amoxicillin-clavulanate. We reviewed charts to compare the response rate between the two different antibiotic treatments. We hypothesize that they will be equally effective and thus the approach that yields higher compliance would be the recommendation. Table 1 Methods Table 2 Conclusions The study did show there was no statistically significant difference between the two studies, yet was under powered to show clinically significant efficacy between the two medications for treatment of sinusitis. The dilemma came with the relatively difficult of ensuring follow ups in a majority of these patients. A larger population would be required to show that the two treatments are equivocal. During the course of my investigation a more recent 2012 IDSA guidelines for diagnosis and management of bacterial sinusitis was released and it changed the initial antimicrobial therapy recommendation to “low dose” amoxicillin-clavulanate (45 mg/kg/day) and recommended “high dose” amoxicillin-clavulanate (90mg/kg/day), clindamycin, a cephalosporin or a flouroquinalone as second line therapy. Macrolide therapy is no longer recommended due to high rates of resistance. [13] Although there are studies that showed compliances can be reported to correlate with dosing frequency 80% for once-daily regimens to 60% for twice-daily.[14] Also this study showed of the patients that started amoxicillin-clavulanate 7% had adverse reactions which stopped treatment, as compared to 0% for azithromycin. Of the adverse reactions seen in the Henry et al study 8.9 % of amoxicillin-clavulanate discontinued treatment due to adverse events, compared to 5.7% of those treated with azithromycin. [11] While this study did have a lower clinical success rate of cure than most studies, it involved patients who already had been treated with an antibiotic recently and failed the course and therefore were more likely to have a resistant organism. With the frequency at which we give antibiotics, a more clarified understanding of second line treatments should be looked at in a larger study prospective study. Given azithromycin ease of use and lower adverse reaction rate, it can still be considered as part of the treatment in sinusitis. References 1 Shapiro, DJ, Gonzalez R, Cabana MD, et al. National trends in Visit Rates and Antibiotic Prescribing for Children with Acute Sinusitis. Pediatrics 2011;127;28-34. 2 Lusk RP, Stankiewicz JA. Pediatric rhinosinusitis. Otolaryngol Head Neck Surg. 1997; 117: S53-S57. 3 Aitken M, Taylor JA. Prevalence of clinical sinusitis in young children followed up by primary care pediatricians. Arch Pediatr Adolesc Med. 1998; 152:244-248. 4 Ueda D, Yoto Y. The ten-day mark as practical diagnostic approach for paranasal sinusitis in children. Pediatr Infect Dis J. 1996; 15: 576-579. 5 Wald ER, Guerra N, Byers C. Upper respiratory tract infections in young children: duration of and frequency of complications. Pediatrics. 1991; 87:129-133. 6 McCaig LF, Hughes JM. Trends in antimicrobial drug prescribing among office-based physicians in the United States [published erratum in JAMA. 1998; 11:279]. JAMA 1995; 273:214-219 7 American Academy of Pediatrics, Subcommittee on Management of Sinusitis and Committee on Quality Improvement. Clinical practice guideline: management of sinusitis [published corrections appear in Pediatrics. 2002; 109(5): 40 and Pediatrics 2001; 108 (5): A24]. Pediatrics. 2001; 108(3): 798-808. 8 Wald ER. Sinusitis. Pediatr Ann. 1998; 27:811-818. 9 Karma P, Pukander J, and Penttila M. Azithromycin concentration in sinus fluid and mucosa after oral administration. EurJ Clin Microbiol Infect Dis. 1991; 10: 856-859. 10 Pichichero ME. Short course of antibiotic in acute otitis media and sinusitis infections. J int Med Res. 2000; 28: 25A-36A. 11 Henry DC, Riffer E, Sokol WN et al. Randomized double-blind study comparing 3- and 6-day regimens of azythromycin with a 10-day amoxicillin-clavulanate regimen for treatment of acute bacterial sinusitis. Antimicrobial Agents and Chemotherapy. 2003; 47(9): 2770-2774. 12 NG D, Chow P, Leung L et al. A randomized controlled trial of azythromycin and amoxicillin-clavulanate in the management of subacute childhood rhinosinusitis. J Peadiatr Child Health. 2000; 36: 378-381. 13 Chow AW, Benninger MS, Brook S et al. IDSA clinical practice guidelines for acute bacterial rhinosinusitis in children and adult. Clinical Infectious Diseases. Advance Access March 20, 2012: e1-e41. http://www.idsociety.org/uploadedFiles/IDSA/Guidelines-Patient_Care/PDF_Library/IDSA%20Clinical%20Practice%20Guideline%20for%20Acute%20Bacterial%20Rhinosinusitis%20in%20Children%20and%20Adults.pdf. 14 Sclar, D. A., T. A. Tartaglione, and M. J. Fine. Overview of issues related to medical compliance with implications for the outpatient management of infectious diseases. Infect. Agents Dis. 1994. 3:266–273. Graph 1 2013 Texas Pediatric Society Electronic Poster Contest Insert Program or Hospital Logo

![[Insert Hospital Name]](https://cdn0.slideserve.com/59021/insert-hospital-name-dt.jpg)

![[Insert Client Logo]](https://cdn1.slideserve.com/1968686/slide1-dt.jpg)

![[Insert Client Logo]](https://cdn1.slideserve.com/2208608/slide1-dt.jpg)