Download
1 / 13
300 likes | 1.13k Views
Chest Injuries. Main Causes of Chest Trauma. Blunt Trauma - Blunt (direct) force to chest. Penetrating Trauma - Projectile that enters chest causing small or large hole. Compression Injury - Chest is caught between two objects and chest is compressed. Chest wall injuries. Rib fractures

E N D
Main Causes of Chest Trauma • Blunt Trauma- Blunt (direct) force to chest. • Penetrating Trauma- Projectile that enters chest causing small or large hole. • Compression Injury- Chest is caught between two objects and chest is compressed.
Chest wall injuries • Rib fractures • Flail chest • Open pneumothorax
Rib fractures • Most common thoracic injury which characterized by Localised pain, tenderness. • Upper ribs (mainly three pairs), clavicle , sternal or scapula fracture indicate sever trauma and may be associated with spinal injury or vascular damage . • With lower rib fractures, abdominal visceral injury, such as liver, spleen or kidney, may occur. Sternalfracture. Fractureoftheleftfirstrib.Thisinjury isassociatedwithanincreasedincidenceof neurovascularinjury,in thesubclavianvein.
Open Pneumothorax • Opening in chest cavity that allows air to enter pleural cavity. • A common complication of chest trauma (15–40%). Causes the lung to collapse due to increased pressure in pleural cavity • Can be life threatening Signs and symptoms Simple pneumothorax: the edge of the right lung is clearly seen (arrows) devoid of peripheral lung markings. No mediastinal shift occurs. • Dyspnoea • Sudden sharp pain • Subcutaneous Emphysema • Decreased lung sounds on affected side
Flail chest • A condition of multiple rib fractures produce a mobile fragment which moves paradoxically with respiration • Usually traumatic with two or more ribs fractured in two or more places.. • Always consider underlying lung injury (pulmonary contusion). • Underlying lung contusion are likely to contribute to the patient’s hypoxia. • The main Clinical features are: Dyspnoea, Tachycardia, hypoxia ,Cyanosis and Hypotension
Haemothorax • Occurs when pleural space fills with blood • Usually occurs due to lacerated blood vessel in thorax • As blood increases, it puts pressure on heart and other vessels in chest cavity • General increased opacification of the hemithorax is seen on a supine film • Ruptured major airway: • This should be suspected in the presence of any of the following : • haemoptysis , • collapse of the lung or lobe, • Pneumothorax with major air leak. Rupture diaphragm: This is more characterized with a bowel or stomach shadow in the thoracic cavity or an ill defined hemi diaphragm.
Diaphragm Rupture Haemo-thorax The opacification of the left hemithorax is du to a haemothorax. A tear in the Diaphragm that allows the abdominal organs enter the chest cavity
Chronic obstructive pulmonary disease ●General term of conditions including chronic bronchitis and emphysema. ● Characterised by chronic airflow reduction resulting from resistance to expiratory airflow, infection, mucosal oedema , bronchospasm and bronchoconstriction . ● Causative factors include smoking, chronic asthma and chronic infection CXRs In the emergency setting, useful for assessing complications, such as pneumonia, heart failure, pneumothorax or rib fractures. – Radiographic features include hyper-expanded (enlarged) lungs associated with flattening of both hemidiaphragms The lungs are hyper-inflated with flattening of both hemi-diaphragms
Aortic rupture • Usually blunt trauma involving Chest; especially RTAs or fall from a height ~80-90% die within minutes • clinical suspicion, CXR, aortography and contrast CT are done • An aortic rupture should be suspected from the mechanism of injury. • Chest or inter-scapular pain will be present. Traumatic aortic rupture: tracheal deviation to the right; left haemothorax, blurring of the outline of the aortic arch. Rib fractures and a traumatic left diaphragmatic hernia are also noted.
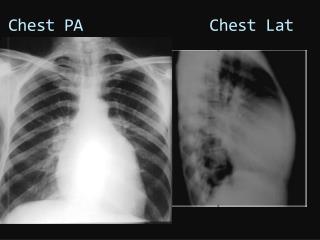
Radiographic projections of the chest Postero anterior : It is used commonly for all cases unless the patient requires ongoing assessment , resuscitation , treatment , or monitoring. Anteroposterior : This view is usually requested for seriously ill patients with a life threatening condition that requires assessment , monitoring , or treatment in a resuscitation area. Lateral chest film: The lateral chest radiography is rarely helpful in acute conditions. However , it can localize abnormalities seen in the postero anterior view. PA )patient with pericadial effusion Lateral decubitus film: It can identify a small pleural effusion and differentiate this from pleural thickening . A sub-pulmonary haemothorax may become apparent with this view when the only abnormality seen in the postero anterior film is a raised hemi diaphragm. Lateral ) patient with air filled mass
Routine Radiographic projections of the chest • Expiration film: • To show a small pneumothorax , • Expiration films are occasionally requested to help establish a diagnosis of inhaled foreign body. • ● inhaled foreign body. • Usually seen in children. • ● Considered an emergency as it may result in complete upper airway obstruction. • If the child is coughing they should be encouraged. • ● the chest may be normal. • Radiological features • ● A radio-opaque foreign body may or may not be seen. • ● secondary signs, such as, segmental collapse, consolidation or hyperinflation, as the foreign body acts as a ball valve.