Download
1 / 49
490 likes | 608 Views
Endocrine Topic. Salyavit Chittmittrapap. Content. 1. Early Metformin Use 2. Correctional & Basal Schedule Insulin 3. Aspirin (no new change) 4. Self monitoring blood glucose (SMBG). How to get ADA2007pdf. Computer ห้องพักแพทย์ In folder “ วิชาการแบ่งตามหน่วย ” Subfolder Endocrine

E N D
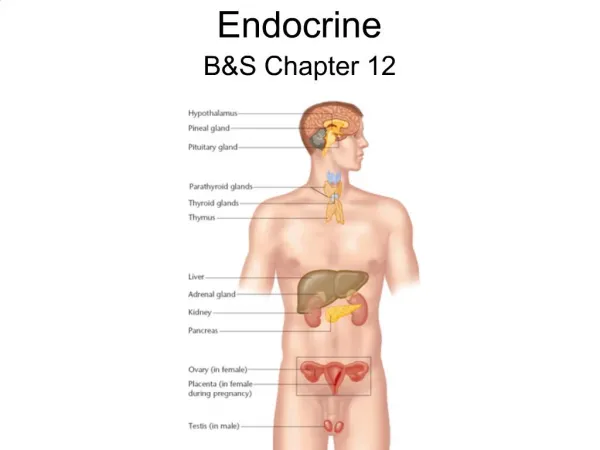
Endocrine Topic Salyavit Chittmittrapap
Content • 1. Early Metformin Use • 2. Correctional & Basal Schedule Insulin • 3. Aspirin (no new change) • 4. Self monitoring blood glucose (SMBG)
How to get ADA2007pdf • Computer ห้องพักแพทย์In folder “วิชาการแบ่งตามหน่วย” Subfolder Endocrine • Download from Diabetes Care Websitecare.diabetesjournals.org/ • และจะ Upload เอาไว้ที่Website ของภาควิชา
Content of ADA CPR 2007 • Standard of Medical Care in DM 2007 • Diagnosis and Classification of DM • Nutritional Recommendation for DM • Nutritional Intervention for DM What's new
4 3 1 2
Evidence grading (adapted) • A – best ; good RCT !, Meta-analysis, compelling nonexperimental evidence • B – good Cohort study, meta of Cohort, good Case-control study • C – poorly controlled / uncontrolled study observational study, poor RCT, case-series, Conflicting evidence! • E – Expert consensus Not Level of Recommendation
Revised Position statement 1 • Nutrition Recommendations and Interventions for Diabetes: A position statement of the American Diabetes Association • American Diabetes Association Diabetes Care 2007 30: S48-65. • Comprehensive Table3 at pageS58-60
2 Diabetic Peripheral Neuropathy RX
Summary of Revision * * * 3 • Diabetes Care • Comprehensive diabetes evaluation revised • Lowering A1C has been assoc. with a reduction of microvascular & neuropathic complication (A) & possibly macrovascular disease (B) • Medical Nutrition Therapy (MNT) extensively revised
Summary of Revision * * * Nephropathy 3 • Reduction of protein intake to 0.8-1.0 g/kg BW /day in pt. with DM & earlier stage of CKD & to 0.8 g/kg BW /day in the later stage of CKD may improve measure of renal function & is recommended (B) • Celiac disease (child)
Summary of Revision * * * DM care in the hospital 4 • Using correction dose or “supplemental” insulin to correct premeal hyperglycemia in addition to scheduled prandial and basal insulin is recommended (C) • Discontinue ACEI before conception (E) • Diabetes care in the school & day care setting should use a plan (504 plan)by family, school nurse, diabetes health care team
Diabetes Mellitus • Is Chronic illness • Need Continuing medical care • Patient self-management education • Prevent acute complication • Reduce the risk of long-termcomplication
Start with MetforminDon’t wait a second Nathan ET.AL Management of Hyperglycemia in type 2 diabetes consensus statement from ADA and EAstudy of DM. Diabetes Care 29:1963-1972 2006
Target HbA1c <7 % • Keep < 7 % • Reconsider in patient with Short Life expectancy & Terminal illness • Some individual patient benefit from keep HbA1c < 6 % • *with higher Hypoglycemia risk *
After Insulin useDiscontinue Sulfonylurea (or decreased dose)
Thiazolidinedione • After titration of Dose Patient may end up with (Maximal medication) = Intensive insulin with MFM • With or without thiazolidinedione • Actos (15) =42 baht • Avandia (4) =64.5 baht • ADR= fluid retention, Weight gain
Manual adjust Sliding Scale • จริง ๆ แล้วดี เพราะมีการคิดแบบ individual case มองทั้ง insulin maintenance และการตอบสนองต่ออินซูลินครั้งก่อน ๆ • แต่ไม่ดีเพราะแพทย์เจ้าของไข้ไม่ได้อยู่เวรทุกวัน และไม่มีมาตรฐานกลางในการการปรับเปลี่ยนขนาดของอินซูลิน • ไม่ดีเพราะไม่มีการปรับเปลี่ยนขนาดของอินซูลิน ในแต่ละวัน • ทำให้เกิดน้ำตาลสูง / ต่ำ เมื่อ insulin requirement เปลี่ยนแปลง
Correctional dose & Schedule Insulin • เมื่อนำ sliding scale มาปรับปรุงเพิ่มโดยปรับเพิ่ม-ลดในแต่ละวัน ก็ได้เป็น correctional & schedule insulin • มีปริมาณ Basal schedule Insulin คือปริมาณที่คนไข้ที่ระดับน้ำตาลปรกคิต้องการ เป็น maintenance dose • มีการเพิ่มหรือลดปริมาณ insulin ที่ฉีดตามปริมาณน้ำตาลตั้งต้น (DTX) • และสามารถปรับเพิ่มหรือลด scale ตามผลการควบคุมน้ำตาลที่ผ่านมา โดยปรับที่ basal insulin
Correctional dose & Schedule Insulin • Continuous Order • If DTX <60,or >291 please notify • DTX 61-80 decrease insulin 4 u • DTX81-100decrease insulin 2 u • DTX 100-140 no modification • DTX 141-170 increase insulin 2 u • DTX 171-200 increase insulin 4 u • DTX 201-230 increase insulin 6 u • DTX 231-260 increase insulin 8 u • DTX 261-290 increase insulin 10 u • One day Order • RI 10 – 10 – 10 sc ac • Monotard 10 u sc hs.
Example . DM male 55yrs on oral feeding • Previously need total insulin 40 u /day • Start with 10 u basal insulin • DTX morning 145 RI 12 u • DTX noon 70 RI 6 u • DTX evening110 RI10 u • DTX hs90 Monotard 8 u • Continuous Order • DTX 61-80 decrease insulin 4 u • DTX81-100decrease insulin 2 u • DTX 100-140 no modification • DTX 141-170 increase insulin 2 u • DTX 171-200 increase insulin 4 u • DTX 201-230 increase insulin 6 u • One day Order • RI 10 – 10 – 10 sc ac • Monotard 10 u sc hs. • TOTAL TODAY 36
Example . DM male 55yrs on oral feeding • Previously need total insulin 40 u /day • Start with 10 u basal insulin • DTX morning 145 RI 12 u • DTX noon 190 RI 14 u • DTX evening180 RI14 u • DTX hs220 Monotard 16 u Correctional Insulin 16 u thenIncrease Basal inuslin • Continuous Order • DTX 61-80 decrease insulin 4 u • DTX81-100decrease insulin 2 u • DTX 100-140 no modification • DTX 141-170 increase insulin 2 u • DTX 171-200 increase insulin 4 u • DTX 201-230 increase insulin 6 u • One day Order • RI 10 – 10 – 10 sc ac • Monotard 10 u sc hs. • TOTAL TODAY 56
Benefit • Hypoglycemic Symptom = Hypoglycemia ? • Better Glycemic control • Cost ; ค่าเครื่อง (1800) • ค่าแถบตรวจน้ำตาล (9) • สำคัญกว่าคือใช้ให้ได้ประโยชน์ DM type 1 GDM
Thailand situation; Beware ! • Increased RISK OF BLEEDING • NSAID abuse • Regular NSAID uses • Untreated Peptic Ulcer • Uninvestigated Dyspepsia • Undetected (&Untreated H.Pylori)
Landmark Paper for starting metformin immediately after Diagnosis of DM
OGTT is bettertest with much complicated steps , used limitedly eg. After IFG
GDM • Develop DM after Pregnancy = overt DM • Different number from harrison Harrison target Fasting <105 Post Prandial <120
High Risk modest wt. loss, regular physical activity. Esp with IGT*** (A) • For IFG same (E) • Follow up counseling appears to be important for success (B) • Monitor DM in pre-DM q 1-2 years (E) • No Medication !!!
Reduce Risk & Slow progression of DN by Blood Pressure & Glucose control (A) • Screen Microalbuminuria annually • - type 1 ; 5yrs or more after DX • - type 2 ; at DX • - during Pregnancy (E) • Screen serum Cr annually(E)
ACEI & ARB • No Winner !!!
If cannot use ACEI & ARB ; Betablockers, Diuretics, Non-DCCBs is considered(E) New Check K
Reduce Risk & Slow progression of DR by Blood Pressure & Glucose control (A) • ASA does not prevent DR nor increase the risks of hemorrhage (A) • Screen by Opthalmologist or Optometrist • Screen annually ; start at • - type 1 ; 3-5yrs or more after DX • - type 2 ; at DX (B) Pregnant = risk progress DR Check DR at preg, along and 1yr post partum
A. Cardiovascular Diseases • 1. BP control • 2. Dyslipidemia • 3. ASA (detail=above) • 4. Smoking cessation • 5. CHD screening & treatment
=Plasma glucose <70 mg/dl • Repeat after RX at 15 min (B) • Glucagon use (E)
K. Immunization • Annual Influenza virus (C) • One (lastlong) Pneumococcal Vaccine • Repeat if >65 yrs with recent vaccine >5 yrs • Repeat if Nephrotic Syndrome, CKD, immunocompromised state
Take Home Message • You should start Metformin after dx DM • Correctional dose & Schedule Insulin • DM+DN ; diabetic diet, Protein 0.8-1.0 g/kgBW/d(0.8 for Late CKD), low fat • Advice symptom of DKA-HHS and also Stroke & MI • ASA gr.I 2*1 with discussion of benefit & risk