Download
1 / 33
381 likes | 723 Views
Mycobacterium leprae. Leprosy: Chronic infectious disease Caused by Mycobacterium leprae - an acid fast bacillus. Mainly affects the skin, peripheral nerves, and mucosa of the respiratory tract etc.

E N D
Leprosy: • Chronic infectious disease • Caused by Mycobacterium leprae - an acid fast bacillus. • Mainly affects the skin, peripheral nerves, and mucosa of the respiratory tract etc. • It has left behind a terrifying image in history and human memory of mutilation, rejection and exclusion from society.
History of Leprosy • Mycobacterium Leprae - first observed by Hansen in 1873 • Leprosy was known since ancient times • First bacterial pathogen of humans to be described, but least understood
Mycobacterium leprae: • Obligatory intra-cellular parasite • Non-cultivable in vitro • Humans and Armadillos are only known natural hosts • Mycobacterium lepraremultiplies very slowly
Slightly curved acid fast bacillus • 5% Sulphuric acid used for decolorisation • Live bacilli appear uniformly stained • Dead bacilli – fragmented and granular • Seen singly or in clumps (GLOBI) intracellularly or outside the cells
Signs of Leprosy • Definite loss of sensation in a skin lesion consistent with leprosy • Skin smears positive for acid fast bacilli • Thickening of one or more peripheral nerves
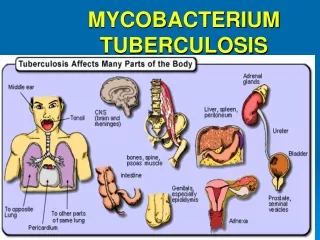
Attacks the cooler areas of the body • Destroys neurons in these areas – altered sensation • Leprosy also causes cartilage in those areas to get absorbed back into the body, causing destruction of fingers, toes, ears and nose • Leprosy also causes large bumps in the skin that do not feel pain and do not heal
Classification of leprosy: • Ridley-Jopling classification • Depending upon – Skin lesions – Bacterial load – Histology • Tuberculoid Leprosy (PB) • Borderline Tuberculoid Leprosy (BT) • Borderline borderline Leprosy (BB) • Borderline lepromatous Leprosy (BL) • Lepromatous Leprosy (MB)
WHO Classification – Paucibacillary (2-5 skin lesions) – Multibacillary (>6 lesions) • Paucibacillary (PB) Leprosysymptoms are: • Well defined skin lesions that are numb • Multibacillary (MB) Leprosysymptoms are: • Chronically stuffy nose and many skin lesions and nodules on both sides of the body
Types of leprosy • Lepromatous leprosy : damages respiration, eyes, and skin • Tuberculoid leprosy: affects nerves in fingers and toes, and surrounding skin • Borderline leprosy: has effects of both types
Transmission Human to human transmission • Nasal discharge • Close contact with skin lesions of patients
Pathogenesis…………………. • Leprosy is a chronic granulomatous disease • Only source of infection is the patient Pathology is determined by the immune response • That causes damage to peripheral nerves • May result in disability and deformity
M.leprae within the new host • Brief bacteraemic phase • Binds to skin macrophages and Schwann cells • Elicits immune response • Development of host protective immunity or progression to established leprosy • Long incubation times • 2-5 years tuberculoid • 8-11 lepromatous
Antigenic structure: • Cell wall of M.leprae – 4 layers • Innermost – Peptidoglycan – shape & rigidity • Lipoarabinomanan-B (LAM – B) • Mycolic acid layer • Mycosides –outermost layer – containing phenolicglycolipid(PGL-1) • LAM-B – highly immunogeneic • PGL-1- protects bacteria against host cell CMI
What are the signs and symptoms? • Large nodules on the skin that do not feel pain • Large ulcers on the skin that do not heal for weeks or months • Muscle weakness • Disappearance of eyebrows or eyelashes
Nerve damage • Occurs across the spectrum • Occurs before diagnosis, during and after treatment Skin • Sensory and autonomic nerve fibres • Peripheral Nerve Trunks • Motor weakness • Regional sensory loss
SUSPECT CASE OF LEPROSY • One or more suggestive skin patches with normal sensation • Extensive loss of sensation in the hands or feet with no other evidence of leprosy • One or more grossly enlarged peripheral nerve trunks with no sensory loss or skin lesion • Painful nerves with no other evidence of leprosy • Painless ulcers on hands and/or feet with no other evidence of leprosy • Nodules on the skin with no other evidence
Diagnosis of Leprosy • History • Clinical Examination • – Skin lesions • – Thickened nerves • Slit skin smears/histology
Specimens: • Split skin smears from: Mucosa, skin lesions & Ear lobules • Acid fast staining : Smears are graded based on the No. of bacilli • BACTERIOLOGICAL INDEX • MORPHOLOGICAL INDEX • Skin and nerve biopsy • Lepromin test
Treatment of leprosy • Treat the infection • Treat reactions and nerve damage • Prevent neuropathic damage • Education • Psychological support • Reduce stigma
Multiple Drug Treatment (MDT) • Effective chemotherapeutic agents: • Dapsone (diaphenylsulfone, DDS), • Rifampicin (RFP), • Clofazimine (CLF), • Ofloxacin (OFLX), • Minocycline (MINO)
Treatment of Paucibacillary leprosy: • Maximum period of 9 months • Rifampicin 600 mg once a month • Dapsone 100 mg every day • Treatment of Multibacillary leprosy: • Maximum period of 18 months • Rifampicin 600 mg once a month • Clofazimine 300 mg once a month • Clofazimine 50 mg and dapsone 100 mg every day
Dapsone (DDS) Rifampicin(RFP) Clofazimine(CLF) • Occasional cutaneous eruptions • A slight reddish coloration of urine, sweat, and tears • Brownish Black discoloration and dryness of skin