Download
1 / 15
150 likes | 310 Views
Crises involving Sexual Assault. Facts & Figures:. Approximately 25% of females and 10% of males will experience sexual assault during their lifetimes. Over 800,000 adult women are raped annually; only about 10% are reported to authorities.

E N D
Facts & Figures: • Approximately 25% of females and 10% of males will experience sexual assault during their lifetimes. • Over 800,000 adult women are raped annually; only about 10% are reported to authorities. • Most perpetrators are men (ages 18-35), while most victims are women and children. • Approximately 30,000 pregnancies result from rape each year. • Approximately 300,000 cases of child sexual abuse are reported each year.
Date Rape: • Approximately 70% of rapes occur between acquaintances (e.g., date rape). • 15-25% of female college students experience rape or attempted rape in the context of a dating relationship. • Victims of date rape may be more likely to have a childhood history of sexual abuse than those who never experience date rape.
Only about 10-15% of victims will seek crisis services immediately after the event; however, many will eventually seek treatment to deal with longer-term consequences from the experience. • Though Rohypnol and GHB get the most attention, alcohol is the #1 date-rape drug and it is frequently present (50-75%) by both the perpetrators and victims of sexual assault.
Conventional View Rape has nothing to do with the rapist’s desire for sex. Rape is an act in which the male gender tries to exert desire for power, domination, and control over all women. Our culture of male supremacy propagates the view that it is acceptable for men to rape women. Evolutionary View Rather than a means of oppressing all women, rape represents the use of violence by a single male against a single female to satisfy a biological desire for sex. A rape that results in the propagation of one’s genes may be biologically adaptive (i.e., the propensity to rape may then be passed to the next generation.) Conceptualization of Rape:
Other Explanations: • Vehicle to express power, control, or domination over victim. • Rape as a form of conquest. • Anger, punishment, or revenge toward victim (may also involve displacement). • Sadistic pleasure. • Taking advantage of an “easy target” (i.e., rapes during wartime). • Recreational rapes (e.g., gang rapes). • Peer pressure.
Stages of Recovery from Rape • Initial Impact: shock/disbelief, emotional & somatic distress, excessive fears (pregnancy, STD’s, being alone), intrusive thoughts, and possibly embarrassment and guilt. • Outward Adjustment: victims appear to be over the rape, but internal problems remain under the surface.
3. Transcrisis Period: stress brings about the return of initial symptomatic stage. 4. Resolution & Integration Period: elimination of psychological distress and self-blame; find meaning in experience and integrate it into one’s personality.
Potential Problems associated with Sexual Assault: • Self-Destructive Behavior (e.g., self-mutilation, promiscuity, drug abuse). • Generalized fear & difficulty trusting others. • Interpersonal & sexual impairment. • Loss of control or helplessness. • Transcrises & PTSD. • Higher risk of re-victimization.
Study by Rind, Tromovitch, & Bauserman (1998) • 27% of females and 14% of males reported CSA. Women were also more likely to experience incest & the use of force. • In general, CSA is weakly associated (r = .04 to .13) with psychological maladjustment. • This relationship basically disappeared after controlling for an index of family environment. Family environment is a better predictor of current problems than CSA. • Contradicting the conventional wisdom, most students who experienced CSA reported no sexual problems. • However, women experienced more negative reactions than men in the sample.
Assessment Issues with Children: • For both legal and clinical issues, complete assessments should only be conducted by human service workers adequately trained in working with abuse victims. • Many of the symptoms experienced by victims of sexual abuse are indistinguishable from symptoms experienced by victims of nonsexual assault or individuals with common psychiatric disorders. • Most distinguishing characteristic: inappropriate sexual behavior.
Frequently, a client’s self-disclosure is the only reliable evidence in a sexual abuse case. • Although false reports of abuse occur and “repressed memories” recovered during therapy may not be accurate, the overwhelming majority of abuse allegations are true.
Risk Factors for Poor Recovery from CSA • Previous, close relationship with perpetrator. • Threat or use of force. • More invasive sexual contact. • Greater duration & frequency of abuse. • Male, compared to female, perpetrator. • Lack of social support, especially from non-offending family members. • Family history of psychopathology and a dysfunctional home environment.
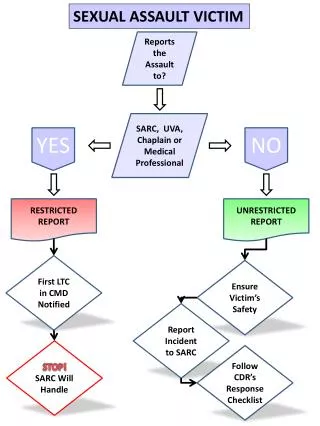
Immediate Crisis Intervention Issues: • Reinforce client for seeking assistance and being a survivor. • Immediate physical & emotional safety of the victim. • Medical evaluation and treatment. • Coordination with legal authorities. • Develop or secure social support. • Refer for psychological evaluation and/or treatment. • Develop a Safety Plan.
Longer-Term Intervention Strategies: • Exposure therapy. • Communication/Assertiveness training. • Reframing & Reattribution of responsibility. • Normalize reactions and subsequent experiences. • Coping Skills Training. • Referral to Self-Help Groups. • Education: sex education, legal information, typical responses to sexual abuse, & PTSD, preventing re-victimization. • Play Therapy & expressive materials for children survivors. • Parent Training.