Download
1 / 62
660 likes | 1.19k Views
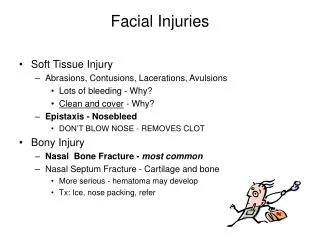
Facial Injuries. Yağmur AYDIN M.D. Associate Proffessor University of Istanbul, Cerrahpasa Medical Faculty Department of Plastic, Aesthetic and Reconstructive Surgery. soft tissue injuries facial bone fractures. Emergency Treatment. Clear Airway and provide patent airway

E N D
Facial Injuries Yağmur AYDIN M.D. Associate Proffessor University of Istanbul, Cerrahpasa Medical Faculty Department of Plastic, Aesthetic and Reconstructive Surgery
soft tissue injuries • facial bone fractures
Emergency Treatment • Clear Airway and provide patent airway • Cleaning of blood, vomit and theet from inside of mouth with fingers • Aspiration of blood, saliva, and gastric contents • Early Intubation or Tracheostomy • Control Hemorrhage • Direct pressure on the wound • Tying of bleeding vessels(a. Facialis, a. Temporalis superfic., a. Angularis, a. Carotis externa) • Angiographic demonstration and embolization of the bleeding point • Anterior-posterior nasal packing • Treat Shock • Evaluate Associated Injuries ( cervical vertebrea, skull base, intracranial, thoracal, intraabdominal) • Diagnosis and treatment of facial injuries
Indications of Tracheostomy • Panfacial fracures(combined mandible, maxilla and nasal fractures) • The multiply fractured mandible with significant swelling of the neck and floor of the mouth • Patients who require prolonged intermaxillary fixation who have significant head or chest injuries • Possibility of prolonged postop. airway problems • Severe facial and neck edema resulting from soft tissue injuries such as severe facial burns • Unrelieved obstruction of airway in the region of larynx or the hypopharynx
Control Hemorrhage Nasal tamponage
Soft tissue Injuries • Laceration(most common form of facial injury) • Contusion (with or without hematoma) • Abrasion • Avulsion • Puncture • Accidental Tattoo • Retained Foreign Bodies
Treatment of Soft Tissue Injuries • Primary closure • Delayed primary closure • Secondary healing • Tertiary healing (skin grafts, flaps)
Wound Closure-I • The time lapse between injury and repair is important in terms of the possibility of infection and the choice of repair techniques • Primary closure is treatment of choice • It is applied immediately after the trauma if the wound is sharp and clean • debridement, excision of a millimeter or two of the wound edge • The wound edges is approximated with sutures
Wound Closure-II • The contused, dirty and heavy contamined wounds are not closed by primaryly • Shotgun wounds, animal and human bites are not closed primarly as well
Delayed Primary Closure • The wound must be prepared with debridment and dressing Cleaning Irrigation Debridment • The wound can be closed primarly after 24-48 hours, If it is clean and free of devitalized tissue
Secondary Closure • If the wound is heavily contamined and infected, contains necrotic and devital tissues after 48 hours, The wound can be closed after cleaning of the wound or can be left to secondary healing • Secondary healing occurs with secondary wound contracture and marginal epithelization
Etiologyof Facial Injuries • Traffic accidents • Interpersonel violence • Spor accidents • Home accidents • Occupational accidents • Shot-gun injuries
Soft tissue Injury Swelling Pain or localized tenderness Crepitation from areas of underlying bone fracture Hypostesia and paralysis in the distribution of specific nerve Malocclusion Class I :Normal oclusion Class II :Retrognathi Class III :Prognathi Visual disturbance Diplopia or decrease in vision Facial asimmetry, deformity Obstructed respiration Lacerations inside of mouth Ecchymosis Bleeding Symptom and Signs
Clinical Examination-I • Evaluation for symmetry and deformity • Inspection of face ( comparing 2 sides) • Palpation of all bony surfaces in an orderly manner (sup. and inf. orbital rims, nose, the brows, the zygomatic arches, malar eminence, border of mandible) • Inspection of intraoral area for lacerations and abnormalities of the dentition • Palpation of dental arches for abnormal mobility
Clinical Examination-II • Maxillary and mandibular dental arches are carefully visualized and palpated for bone irregularity, bruise, hematoma, tenderness or crepitus • Sensory and motor nerve functions in the facial area evaluated • Extraocular movements and muscle of facial expression must be examined • Globe functions (pupillary size and symmetry, globe excursion, eyelid excursion, double vision and visual loss) and fundoscopic examination
Facial Injuries Midface Fractures Le-Fort Maxillary Fractures • Lower Level fractures (Le-Fort I, Transverse, Guerin) • transverse fracture separating the maxillary alveolus from the upper mid face • Upper Level Fractures • Le-Fort II(Pyramidal fracture) : separates a pyramid-shaped central fragment containing the maxillary dentition from the remainder of the orbits and upper craniofacial skeleton • Le-Fort III (craniofacial dysjunction) : separates the maxilla at the level of the upper portion of the zygoma, orbital floor, and nasoethmoid region from the remainder of the upper craniofacial skeleton
Maxillary FracturesSymptoms and Signs • Periorbital hematoma • Nasopharyngeal bleeding • Pain • Swelling on the face • Intraoral lacerations • Malocclusion • Elongation of the face • Maxillary retrusion • Anterior open bite • Abnormal mobility on the dental arc • Rinorea and pneumocephaly (% 25 in LeFort II and III)
Dental Occlusion Normal occlusion Mandibular prognathia Mandibular retrognathia
Imaging • Plain radiographs : Waters’ and lateral view • Axial and coronal CTscans of the midface • 3 D CT Coronal CT Waters’ radiograph 3D CT
Dish-shaped face, loss of facial projection, bilateral conjunctival hemoraji
Goals of treatment restoration of the proper facial aesthetics including preservation of midface width, height and projection
Treatment of Maxilla Fractures Open reduction and intermaxillary fixation and spanning each of the butresses with plate and screws
Orbital Fractures • Classification • Orbital floor blow-out fractures • Pure (nonfractured infraorbital rim) • Inpure (fractured infraorbital rim) • Orbital fractures (without blow-out) • Lineer fractures • Combined with maxillary fractures • Zygomatic fractures
A- small orbital blow-out fracture is confined to the orbital floor B- larger blow-out fracture extends to involve to the lower medial orbit as well as orbital floor Bone graft for repair of medial blow-out fracture
Symptom and Signs • palpebral and subconjunctival hematoma • Diplopia (most common looking superiorly or inferiorly) • Numbness in the inferior orbital nerve distribution • Enophthalmos • Positive forced duction test • Radiological evidence of orbital floor fracture and entrapment of soft tissues on the CT scans with both axial and coronal views • Assessment of the visual system is essential
Coronal CT Orbital Blow-out fracture
Treatment of Orbital Blow-out Fracture • There are two major surgical indications for orbital fracture repair • Muscle entrapment (confirmed by forced duction and CT scan) • volume increase(> 2cm2 defects enophthalmos and globe dystopia developes) • Subciliar or transconjunctival approach • Entrapped soft tissues are brought back from maxiillary sinus • Defect are bridged with bone grafts or alloplastic materials(silicone, titanium mesh, medpor, proplast etc.)
The Superior Orbital Fissure and Orbital Apex Syndrome • ptosis of the eyelid • proptosis of the globe • paralysis of cranial nerve III, IV, and VI • anesthesia in the distribution of the first division of the trigeminal nerve • If blindness occurs in combination with the superior orbital fissure syndrome, the condition is termed the “orbital apex syndrome.”
Nasoethmoidal Orbital Fractures • Symptoms and signs • Telecanthus • Decrease in the dorsal nasal projection • Rinorea • Treatment:open reduction with a combination of interfragmentary wiring and plate and screw fixation
Nasoethmoidal Orbital Fractures and their treatment
Symptoms • periorbital and subconjunctival hematoma • numbness in the infraorbital nerve distribution • epistaxis (ipsilateral or bilateral) • Disturbed occlusion and range of motion of the mandible (inward displacement of the zygomatic arch) • Lack of prominence of the malar eminence
The Physical Signs • periorbital and subconjunctival hematoma, • loss of prominence of malar eminence, • numbness in the distribution of the infraorbital nerve • inferior globe dystopia or enophthalmos • inferior displacement of the palpebral fissure. • Step or level discrepancies may be palpated over fracture sites • tenderness at the sites of the fracture.
periorbital ecchymosis,edema, antimongoloid slant, and subconjunctival hemorrhage.
Worm’s-eye view. Frontal Axial CT scan isolated depressed left zygomatic arch fracture.
The Radiographic Evaluation • Plain films of the Caldwell, Water’s, and submental vertex • Axial and Coronal CT scan
TREATMENT Treatment of zygomatic fracture with Gillies method
Open reduction and rigid fixation with plates and screws at frontozygomatic suture, inferior orbital rim, and zygomatico-maxillary butress
Orbitazygomatic fracture- Repositon and rigid internal fixation
Axial CT Zygomatic Fracture