Download
1 / 46

E N D
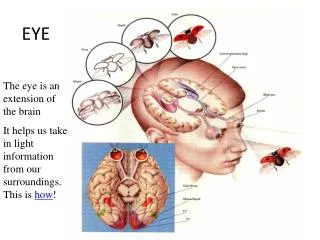
1. EYE EM Adrian Burger
2. How to approach the eye..
3. What do we need? Snellen chart
Magnifier - preferably X8
Torch with a blue filter
Fluoroscine drops or paper
Topical anaesthesia
Topical short acting mydriatic preferably tropicamide
Hand held ophthalmoscope
A Systematic approach
4. Two types Medical - red eye (infection, inflammation)
- loss of vision
Trauma - penetrating
- blunt
- chemical
- thermal
5. History Main symptom(s)
Pain
Discharge
Vision
Any trauma
PMH, PSH
Medication
6. Examination Anatomical
Lymphnodes
Eye movements
Lids and lashes
Conjunctiva
Cornea
Anterior chamber
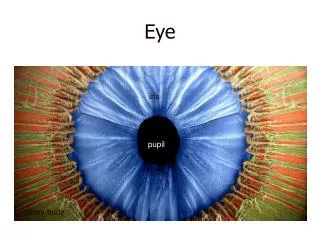
Iris, Pupil & Lens
Fundoscopy
7. Eye Movements
8. Ophthalmoscopy Dim room
Approach from 15cm, �O� magnification
Right to Right, Left to Left
Red reflex
Aim nasally, small aperture, low light
Cornea
Lens
9. Red Reflex
10. Fundoscopy 1 Optic disk
Swelling, cupping
Colour
Vessels, bleeds
Macula
Colour
Exudates, abnormalities
11. Papilloedema
12. Fundoscopy 2 Vessels
New vessels
Tortuousity, segmentation
Colour
Rest of retina
Pallor
Bleeds
Pigmentation
Retinopathy
13. Fundoscopy 3 Tips
Both eyes open � yours and theirs!
Stand to side
Peripheral retina
Dilate pupils - if safe, after RAPD test and
VA test
Polarised filter
14. Rest of exam Visual acuity
Visual fields
RAPD
�Digital� tonometry
15. VA � Pinhole
16. Rest of exam
17. Lids and Lashes
18. Lacrimal System
19. Dacryocystitis Treatment Acute - antibiotics
- I & D
Chronic - DCR
20. Lids and lashes
21. Viral
22. Viral treatment Check Cornea!
Symptomatic, supportive
Chloramphenicol
Refer if in doubt
23. Bacterial
24. Bacterial Treatment Simple - chloramphenicol
- drops day, ointment nocte�
Gonococcal - admit
- swabs
- IV cefoxitin 1g QID
- Topical Gentamycin
Neonatal - IV and topical Pen
Chlamydia - occ. Tetracycline QID four weeks
- Oral doxycycline or erythromycin
for six weeks
25. PKC HS reaction
Self resolving
?Steroids
26. Allergic, Vernal, GPC
27. Treatment Topical Antihistamines
Spersallerge �
Topical Mast cell stabilisers
Optichrom �
Topical Steroids
Refer
28. Conjunctiva - other
29. Cornea
30. HZO Refer
Check immunity
Treat
Systemic antivirals
Topical antivirals
Analgesia
31. Glaucoma
32. Acute Angle Closure
33. Glaucoma Post - Surgery
34. Chronic OAG Cup/disk ratio
35. Acute Angle Closure Mx Recognise
Risk or reality
Meds - diamox 500mg stat, 250mg QID
- glycerine/mannitol 1-2g/kg
- pilocarpine 1-2% QID
- B-blockers BD
Referral for Laser or Surgery
36. Diabetic retinopathy Background - dot and blot
- hard exudates
Pre-proliferative - cotton wool spots
- IRMA
- venous segmentation
- large dark blots
Proliferative - NVD or NVE
- vitreous bleeds
- fibrous proliferation and retinal detachment
- neovascular glaucoma
37. Non Proliferative Background
- dot and blot
- hard exudates
-micro aneurysms
- macular oedema
Pre-proliferative
- cotton wool spots (soft)
- IRMA
- venous segmentation
- large dark blots
38. Proliferative NVD
NVE
Fibrovascular proliferation
Vitreous bleeds
39. Proliferative 2
40. FB, Blunt and Perforating Trauma
41. Blunt Trauma
42. Corneal Injury
43. Lens Injury
44. Other trauma Traumatic mydriasis
Traumatic iritis
Vitreous bleed
Retinal detachment
Macula oedema
Optic neuropathy
45. Trauma management Analgesia
Low light
Gentle
Same as all eyes
X rays
Topical antibiotics
Tet Tox
46. References UCT Ophthalmology Lecture Notes
www.trauma.org
www.medicine.ucsd.edu/clinicalmed/eyes.htm
www.atlasophthalmology.com
www.eyecasualty.co.uk
www.webeye.ophth.uiowa.edu/eyeforum