Download
1 / 80
860 likes | 1.02k Views
Understand renal system differences, diagnostic investigations, common disorders, and nursing management in children. Learn pediatric kidney development and functions of nephron and kidney. Discover diagnostic procedures for genito-urinary issues.

E N D
DISORDERS OF THE GENITO-URINARY SYSTEM IN CHILDREN
Aim To show an in-depth understanding of the genito-urinary disorders in children and the process of care in the nursing management
Learning Objectives By the end of this session, the student should be able to: • Understand the anatomy and physiology of the renal system and structure and function • Identify the differences between adult and children GU system • Describe the most common diagnostic investigations and procedures for GU disorders
Learning Objectives…con’t • Understand the general assessment of children with genitourinary disorders • Understand the common genitourinary disorders in children • Plan the nursing management for children with GU disorders
PAEDIATRIC DIFFERENCES OF KIDNEY DEVELOPMENT • Begins during 1st week of gestation • Completed by end of 1st year after birth • Excretion less than adult • By the age of 6 to 12 months, filtration and absorption is nearly like adults • For healthy infant, the kidneys operate at a functional level appropriate for the size of the body.
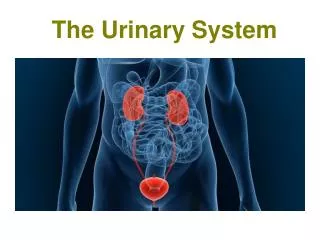
Function of Kidney Nephron • Glomeruli – filter water and solutes from blood • Tubules – reabsorb needed substances (water, protein, electrolytes, glucose, amino acids) from filtrate and allow unneeded substances to leave the body in urine • Urine formed in the nephron, passes into renal pelvis, through ureter into bladder and out of body through urethra
Urine formed in the nephron, passes into renal pelvis, through ureter into bladder and out of body through urethra
Glomeruli : filter water and solutes from blood Tubules : reabsorb needed substances (water, protein, electrolytes, glucose, amino acids) from filtrate and allow unneeded substances to leave the body in urine
Function of Kidney • Maintaining body fluid volume and composition • Secretes hormones:- • Renin – helps with the regulation of blood pressure • Erythropoietin – stimulates red blood cell production by the bone marrow • Metabolised Vitamin D – responsible for calcium metabolism
Diagnostic Investigations • Urinalysis • CT Scan- an x-ray procedure that combines many x-ray images with the aid of a computer to generate cross-sectional views and, if needed, three-dimensional images of the internal organs and structures of the body.
Blood urea nitrogen (B.U.N) and creatinine - • gross indicator of renal function • (BUN) test measures the amount of nitrogen in blood that comes from the waste product urea. • Urea is made when protein is broken down in body. • Blood urea nitrogen (BUN) and creatinine tests can be used together to find the BUN-to-creatinine ratio (BUN:creatinine). body in the urine. • A blood urea nitrogen (BUN) test is done to determine : • kidneys are working normally. • kidney disease is getting worse. • See if treatment of kidney disease is working. • See if severe dehydration is present. Dehydration generally causes BUN levels to rise more than creatinine levels. This causes a high BUN-to-creatinine ratio. Kidney disease or blockage of the flow of urine from kidney causes both BUN and creatinine levels to go up.
Cystoscopy – bladder and urethra are examined with cystoscope (fibre optic technology)
KUB (Kidney, Ureter, Bladder) x-ray • Renal Biopsy Renal Ultrasound
Intravenous pyelogram (IVP) An injection of x-ray contrast media via a needle or cannula into the vein, typically in the arm. The contrast is excreted or removed from the bloodstream via the kidneys, and the contrast media becomes visible on x-rays almost immediately after injection
Retrograde Pyelogram • a urologic procedure where the physician injects contrast into the ureter in order to visualize the ureter and kidney. • Micturating Cystourethrography (MCUG) – serial x-ray of the bladder and urethra after IV infusion of iodine-bound contrast medium ( to detect blockage)
COMMON DISORDERS OF THE GENITOURINARY SYSTEM • Urinary tract infection (UTI) • Nephrotic syndrome • Acute Post-Streptococcal Glomerulonephritis (APSGN) • Vesicoureteral reflux • Hypospadias
URINARY TRACT INFECTIONS Definition • UTI is the presence of bacteria in the urine • Infection usually occur at the upper urinary tract or at the lower urinary tract Incidence • Common age of onset for UTI is 2-6 years • Girl>Boy - Female has shorter urethra • Uncircumcised male prone to develop UTI
Causes • Causative organisms – E. Coli • Route of entry -bacteria ascending from the area outside of the urethra. • Vesico-ureteral reflux • Infections – URTI, GE • Poor perineal hygiene - fecal organisms are the most common infecting organisms due to the proximity of the rectum to the urethra. • Short female urethra
Types of UTI • Urethritis – infection of the urethra • Cystitis – an infection in the bladder that has moved up from the urethra • Pyelonephritis – a urinary infection of the kidney as a result of an infection in the urinary tract
Unexplained fever (febrile fits) Poor growth Abdominal pain Foul-smelling urine Signs & Symptoms of UTI in babies Irritability Poor feeding Weight loss (failure to weight gain) Vomiting
Signs & Symptoms of UTI in older children • Nausea and vomiting • Low abdominal or flank pain • Fever and chills • Fatigue • Small amount of urine while micturating despite feeling of urgency • Urinary frequency/urgency • Dysuria • Foul-smelling urine • Cloudy urine • Incontinence during day and/or night • Increased irritability
Signs of serious infections • Central pyrexia but peripherally cold • Poor colour • Pale, grey mottled skin • Quiet and lethargic child • Poor tone • Tachycardic and hypertensive
Diagnostic investigations • Obtaining a urine specimen:- - Urine bag - Clean catch urine - Mid-stream urine - Catheterisation - Supra-pubic aspiration-draining the bladder by inserting a sterile needle through the skin above the pubic arch and into the bladder.
Diagnostic investigations • Ultrasound • Plain x-ray • MicturatingCystourethrogram (MCUG)
Nursing care • Obtain urine specimen before antibiotics started, sent for ME/CS • Blood tests • Strict I/O chart • Monitor vital signs esp. body temperature • Administer antibiotics as prescribed (5 days course) • Administer anti-pyretic drugs to reduce fever and pain • Advised to take plenty of fluids to prevent dehydration and to flush the urinary tract • If the child is unable (vomiting) or refuse to take fluids, administer IV fluids as prescribed
Nursing Problems • Fever due to increased body temperature related to urinary tract infection. • Alteration in urination (frequency, pain, burning, dribbling and enuresis) related to infection. • Pain related to inflammatory changes in the urinary tract. • Lack of knowledge about UTI and health prevention
Problem 1: Fever due to increased bodytemperature related to urinary tract infection Goal: to reduce fever and maintain normal body temperature
Problem 2: Alteration in urination (frequency, pain, burning, dribbling and enuresis) related to infection Goal: to ensure that the child is comfortable during urination
Health teaching to prevent UTI • Ensure the child to pass urine regularly (every 2-3 hours) and take the time to completely empty the bladder • Avoid holding urine for prolonged period of time • Perineal hygiene - wipe from front to back • Avoid tight fitting clothing or diapers; wear cotton panties • Avoid constipation • Encourage fluid intake • Avoid bubble baths
Student’s Activity You are required to do the nursing care plan for problem no. 3 & 4, including nursing interventions and rationales
Nephrotic Syndrome Nephrotic Syndrome
What is Nephrotic Syndrome? • Alteration of glomerular membrane permeability with massive proteinuria, hypoalbuminaemia, hyperlipidaemia and oedema
Causes • It occurs when the filters in the kidney leak an excessive amount of protein. The level of protein in the blood ↓ and this allows fluid to leak across the blood vessels into the tissues – causing oedema • Nephrotic syndrome are caused by changes in the immune system
Pathophysiology • For unknown reason, the glomerular membrane, usually impermeable to large proteins becomes permeable. • Protein, especially albumin, leaks through the membrane and is lost in the urine. • Plasma proteins decrease as proteinuria increase.
The colloidal osmotic pressure which holds water in the vascular compartments is reduced owing to decrease amount of serum albumin. This allows fluid to flow from the capillaries into the extracellular space, producing oedema. • Accumulation of fluid in the interstitial spaces and peritoneal cavity is also increased by an overproduction of aldosterone, which causes retention of sodium. • There is increased susceptibility to infection due to decreased gamma-globulin. • Causing generalised oedema
Incidence • 1 : 50 000 children • Males > females • Common age of onset is between 2 to 6 years, but can occur at any age
Signs & Symptoms • Oedema - initially noted in the periorbital area - ascites - intense scrotal oedema - striae may appear due to skin overstretching - pitting oedema • ↑ weight • ↓ urine output • Proteinuria (foamy urine indicates proteinuria) • Fatigue • Irritable and depression • Severe recurrent infections • Anorexia • Wasting of skeletal muscles
Diagnostic investigations • Urinalysis - protein 3+ - 4+ on dipstick - haematuria may be absent or microscopic
Diagnostic investigations…con’t • Blood test - total serum protein – low - serum albumin – low - cholesterol and lipoproteins – high • Renal function test – often normal • Blood pressure – often normal but 25% hypertension • Renal biopsy
Nursing problems • Generalised oedema due to fluid volume excess related to glomerular dysfunction • Impaired skin integrity related to oedema • Altered urinary pattern related to glomerular dysfunction • Increased susceptibility to infection related to disease process and steroid therapy
Nursing problems…con’t • Altered body image (round face) due to side-effects of medication • Inadequate nutritional intake related to large loss of protein from the urine • Knowledge deficit of the disease process and treatment • Anxiety and depression due to the up and down of the course of disease
Nursing problem 1 :Generalised oedema due tofluid volume excess related to glomerular dysfunction Goal : to relieve oedema Nursing interventions • Administer steroids – prednisolone 2-4mg/kg to control oedema • Observe for side-effects of steroids – Cushing’s syndrome (moon face, abdominal distension, striae, ↑ appetite, ↑ weight, aggravation of adolescent acne)
Administer diuretic – frusemide. Diuretics can cause loss of electrolytes esp. potassium, encourage ↑ potassium food e.g. citrus fruits, date, apricot, banana • Keep the child CRIB during periods of severe oedema • Strict I/O chart – restrict intake of fluid – offer small amount of measured fluid during severe oedema, for infant measure the diaper’s wt. • Measure daily weight and abdominal girth – to check any weight gain due to water retention
Nursing problem 2 :Impaired skin integrity related to oedema Goal : to protect the child from skin breakdown Nursing intervention • Position the child comfortably in bed so that oedematous skin is well-support with a pillow • Elevate the child’s head to reduce peri-orbital oedema • Provide good skin care – give bath and maintain hygiene esp. genitals and moist area • Change bedding daily and free from creases and sharp objects – to avoid cut