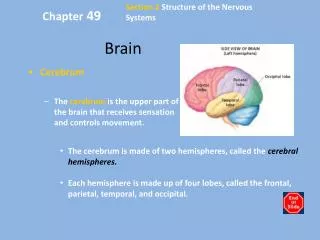
Download
1 / 56
560 likes | 577 Views
Learn about cerebral anatomy, clinical neurosurgery, trauma management, and intracranial pressure. Understand the assessment of motor, sensory, and cerebellar functions. Explore the diagnosis and treatment of various neurosurgical pathologies.

E N D
BRAIN BASICS NESSA TIMONEY MEDICAL CENTER HEALTH BOWLING GREEN KENTUCKY 23 AUGUST 2019
Outline Cerebral Anatomy Clinical Neurosurgery • Diagnosis • Intracranial Pressure • Intracranial Hypertension Management • Clinical Vignettes
Diagnosis of Neurosurgical Pathology GOOD HISTORYAND NEUROLOGIC EXAM MENTAL STATUS EXAM Glasgow coma scale • Eye opening response • Verbal response • Motor response
Diagnosis of Neurosurgical Pathology • CN EXAM • MOTOR EXAM • Pronator drift – must be done on every patient with cranial pathology • If patient slowly drops/pronates hand, it is a sign of contralateral UMN pathology • Tone Rigidity • Grading of Strength – cervical and lumbar • Grade 5: Full strength and resistance • Grade 4: Paritial resistance (may be graded +/-) • Grade 3: Moves limb against gravity • Grade 2: Moves limb but not against gravity • Grade 1: Muscle Twitch
Diagnosis of Neurosurgical Pathology • CEREBELLAR EXAM • Evaluate rapid alternating movements, document any dysdiadochokinesia • Finger to nose to evaluate and underpointing or past pointing indicating dysmetria and ataxic movements • Evaluate tremor (intention, postural, resting, pill rolling) • Romberg test – standing, eyes closed feet together observe for sway or falls • Positive in patients with lesions of one of the 2 sensory systems remaining when eyes are closed (vestibular, proprioception) or in midline cerebellar lesions
Diagnosis of Neurosurgical Pathology • SENSORY EXAM • Light touch and pin prick • Vibratory sensation • DEEP TENDON REFLEXES • Abnormal reflexes - UMN: • Triple flexion: flexion of ankle, knee, and hip • Hoffman’s sign: flexion/adduction of thumb • Babinski sign: upgoing great toe and fanning of toes
Diagnosis of Neurosurgical Pathology Initial Trauma Management: • Primary Survey (ATLS guidelines) • Airway • Breathing • Circulation • Disability • Exposure/Environmental • Secondary Survey • History/Examination
Diagnosis of Neurosurgical Pathology Initial Trauma Management: 3. Physiologic Parameters1 1Guidelines for the management of severe Traumatic Brain Injury 3rd ed.
Diagnosis of Neurosurgical Pathology Labs Coagulopathy vshypercoaguable states Pharmacology: antiplatelet/anticoagulation assays CSF analysis Imaging CT/MRI/Cerebral angiogram
Intracranial Pressure • Monro-Kellie doctrine • Intracranial volume (fixed) = Brain + Blood + CSF • These constituents create a state of volume equilibrium, such that any increase in volume of one of these, must be compensated by a decrease in volume of another • Increased pressure within the cranial cavity is caused by an increase in the volume of either the brain tissue, blood, CSF, presence of a tumor or space-occupying lesion
Intracranial Pressure • Raised ICP is the final common pathway that leads to death or disability in most acute cerebral conditions • Two major consequences of increased ICP are: • Brain shifts • Brain ischemia • Cerebral perfusion pressure (CPP) is the calculated difference between the mean arterial pressure (MAP) and the ICP. • CPP = MAP - ICP
Intracranial Pressure • CPP is the main determinant of cerebral blood flow (CBF) • Normally CBF is coupled to metabolic demand of tissue with normal flow greater than 50 ml/100g/min • Less than 20 ml/100g/min is considered ischemic threshold • The process of cerebral autoregulation maintains CBF between a CPP range of 50 – 150 mmHG • Outside these ranges CBF becomes pressure-dependent
Intracranial Pressure When CPP is less than the lower threshold for autoregulatory compensation, CBF progressively decreases with CPP resulting in ischemia
Space Occupying Lesions • Extra axial lesions – EDH, SDH • Neoplasms • Intraparenchymal hemorrhages • Vascular malformations • Infective pathology: abscess
Clinical Features of Elevated ICP • Cardinal Symptoms: • Headache, vomiting (especially without nausea), papilledema • Cranial Nerve Palsies • Particularly abducens palsies • Cushing response • Arterial hypertension and bradycardia • Abnormal respirations • Cheyne-Stokes – damage to diencephalic region
Clinical Case 3. 76 yo M on aspirin presented with headaches Remote h/o fall 3 weeks prior GCS 15
Chronic Subdural Hematomas • Fluid collection within the layers of the dura mater • 13.1 cases per 100,000 inhabitants • Patients older than 40 years account for 80% of cases – peak incidence 8th decade • Trauma biggest risk factor • Chronic alcoholism/older age predisposition • More falls, treatment with anticoagulation, brain atrophy
Chronic Subdural Hematomas TREATMENT Watch and wait Pharmacological treatment Steroids, ACEI, TXA AEDs Surgery Burr hole vs craniotomy