Download
1 / 47
590 likes | 889 Views
CT BRAIN - BASICS. Dr Mohamed el Safwany , MD. Intended learning outcome. The student should learn at the end of this lecture CT brain basics. CT Principle. RING OF XRAY DETECTORS. Frankfurt plan e. HOUNSFIELD UNITS. Numeric information in each pixel of ct image

E N D
CT BRAIN - BASICS Dr Mohamed el Safwany, MD.
Intended learning outcome The student should learn at the end of this lecture CT brain basics.
CT Principle RING OF XRAY DETECTORS
HOUNSFIELD UNITS • Numeric information in each pixel of ct image • Related to composition & nature of tissue • Represent the density of tissue • Also called as CT NUMBER
CT /MRI • CT PICTURE • WHITE MATTER IS DARKER THAN GREY MATTER SINCE LIPID CONTAINING MATERIAL IS RADIOLUCENT • CSF IS BLACK • MR PICTURE
Step wise approach • Ventricles/ cisterns • Cortex • Deep gray matter • Focal lesions • Bone • Extracranial soft tissue • Para nasal sinuses
LV FRONTAL HORN 3V OCCIPITAL HORN FORAMEN OF MONRO trigone TEMBORAL HORN 4 V AQUEDUCT OF SYLVIUS
ABOVE THE LEVEL OF FORAMEN MAGNUM VA MEDULLA 4 V TONSIL INT OCC PROT
LEVEL OF FOURTH VENTRICLE Optic nerve CPCISTERN TEM HORN PONS 4V MCP
LEVEL ABOVE FOURTH VENTRICLE OLF SULCUS SYLV FISSURE SUPRA SELLAR CISTERN AMB CIST MB 4V vermis
Cerebral Arterial Territory • MCA-most of lateral hemisphere, Basal ganglia, insula, • ACA-Inferomedial basal ganglia,ventromedial frontal lobes, anterior 2/3rd medial cerebral hemispheres, 1 cm supero medial brain convexity • PCA-Thalami, midbrain, posterior 1/3of medial hemisphere, occipital lobe, postero medial temporal lobe
ACA MCA PCA
AICA-inferolateral part of pons, middle cerebellar peduncle, floccular region, anterior petrosal surface of cerebellar hemisphere • PICA-posteroinferior surface of cerebellar hemisphere , ipsilateral part of inferior vermis, • Superior cerebellar artery-superior aspect of cerebellar hemisphere (tentorial surface), ipsilateral superior vermis, largest part of deep white matter including dentate nucleus, pons
Cerebral ischemia • Significantly diminished blood supply to all parts(global ischemia) or selected areas(regional or focal ischemia) of the brain • Focal ischemia- cerebral infarction • Global ischemia-hypoxic ischemic encephalopathy(HIE),hypotensive cerebral infarction
Goal of imaging • Excludehemorrhage • Identify the presence of an underlying structural lesion such as tumour , vascular malformation ,subdual hematoma that can mimic stroke • Identify stenosis or occlusion of major extra- and intracranial arteries • Differentiate between irreversibly affected brain tissue and reversibly impaired tissue (dead tissue versus tissue at risk)
Infarct vspneumbra • In the central core of the infarct, the severity of hypoperfusion results in irreversible cellular damage . • Around this core, there is a region of decreased flow in which either: • The critical flow threshold for cell death has not reached • Or the duration of ischemia has been insufficient to cause irreversible damage.
Hyper acute infarct(<12 hours) • Acute infarct(12 - 48 hours) • Subacute infarct(2 - 14 days) • Chronic infarct(>2 weeks) • Old infarct(>2 months)
CT-Hyperacute infarct • Hyperdense MCA sign-acute intraluminal thrombus • Attenuation of lentiform nulei • Dot sign-occluded MCA branch in sylvian fissure • Insular ribbon sign –grey white interface loss along the lateral insula
CT- Acute infarct • Low density basal ganglia • Sulcal effacement • Wedge shaphed parenchymal hypo density area that involves both grey and white matter • Increasing mass effect • Hemorrhagic transformation may occur -15 to 45% ( basal ganglia and cortex common site) in 24 to 48 hours
CT-chronic infarct • Plain ct • Focal, well-delineated low-attenuation areas in affected vascular distribution • sulci become prominent; ipsilateral ventricle enlarges • Dystrophic Ca++ may occur in infarcted brain but is very rare • CECT: No enhancement
INFARCT / TUMOUR • CLINICAL HISTROY • DISTRIBUTION • SHAPES • GRAY / WHITE INVOLVEMENT • ADVANCED IMAGING
VENOUS INFARCT • HISTROY • BEYOND VASCULAR DISTRIBUTION • HAEMORRHAGIC INFARCT • THORMBUS IN VENOUS SINUSES • SYMMETRICAL LOW ATTENUATION IN DEEP GRAY MATTER - DEEP CEREBRAL VEIN THORMBUS
EDEMA/ INFARCT • INFARCT TYPICAL VASCULAR DISTRIBUTION GRAY MATTER INVOLVEMENT • EDEMA NOT CONFINED TO VASCULAR DISTRIBUTION MOSTLY INVOLVES WHITE MATTER
Text Book David Sutton’s Radiology Clark’s Radiographic positioning and techniques
Assignment Two students will be selected for assignment.
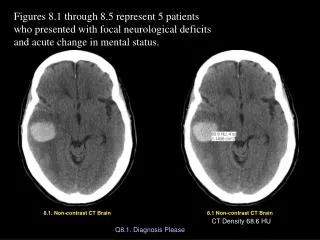
Question Describe CT of acute brain infarction?