Download
1 / 104
1.04k likes | 1.08k Views
T P. UP. A Randomized Trial of Supplemental Parenteral Nutrition in Under and Over Weight Critically Ill Patients : The TOP UP Trial April 12 th 2012 Study Sponsor: Dr. Daren Heyland Project Leader: Rupinder Dhaliwal Project Assistant: Roger Leung Clinical Evaluation Research Unit.

E N D
T P UP A Randomized Trial of Supplemental Parenteral Nutrition in Under and Over Weight Critically Ill Patients: The TOP UP Trial April 12th 2012 Study Sponsor: Dr. Daren Heyland Project Leader: Rupinder Dhaliwal Project Assistant: Roger Leung Clinical Evaluation Research Unit
Point prevalence survey of nutrition practices in ICU’s around the world conducted Jan. 27, 2007 Enrolled 2772 patients from 158 ICU’s over 5 continents Included ventilated adult patients who remained in ICU >72 hours
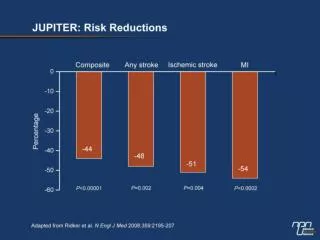
What study patients actually received? Average Calories in all groups: 1034 kcals and 47 gm of protein Result: Average caloric deficit in Lean Pts: 7500kcal/10days Average caloric deficit in Severely Obese: 12000kcal/10days
ICU patients are not all created equal…should we expect the impact of nutrition therapy to be the same across all patients?
TOP UP Trial: Hypothesis Increased early energy and protein delivery with PN+EN to underweight (BMI < 25) and obese (BMI ≥ 35) critically ill patients will result in improved survival at 60 day versus standard EN alone
Objectives • Perform an initial multi-center pilot study in Canada,USA, France & Belgium in 160 patients to demonstrate feasibility • Assuming feasibility, large-scale 2000 patient multi-center, multinational trial will be undertaken
Study Design Randomized Trial (unblinded) EN only Primary Outcome Stratified by: Site BMI Med vs Surg On EN ICU patients R BMI <25 60-day mortality BMI >35 Fed enterally EN plus supplemental PN for 7 days
Objectives: Pilot Study Primary Aim: • Difference in the calories and protein received between the control and intervention groups • Estimate recruitment rate • Evaluate the safety, tolerance, and logistics around providing supplemental PN in the study population, e.g. • To ensure adequate glycemic control in both groups • To ensure other metabolic consequences of the feeding strategies are minimized • To establish adequate compliance with study protocols and completion of case report forms. Secondary Aims: • Explore the effect of differential intake of protein/energy on muscle mass and muscle function.
Outcomes: Pilot study Primary outcome: 60 day mortality Secondary outcomes: • ICU (28 day) mortality • Hospital mortality • Duration of mechanical ventilation • Duration of stay (ICU and hospital) • Development of ICU-acquired infections • Multiple organ dysfunction (SOFA and PODS) • Functional status, HR QOL at 3 & 6 months • Muscle Function Tests
Imp Manual p 9 Study Overview
Pilot Study: Participating Sites Target: 160 patients from 8 institutions • Royal Alexandra Hospital, Edmonton (Jim Kutsogiannis) • University of Alberta Hospital, Edmonton (Dean Karvellas) • University of Colorado, US (Paul Wischmeyer ) • Erasme University Hospital, Brussels (Jean Charles Preiser) • HôpitauxUniversitaires, Strasbourg, France (Michael Hasselmann) • Grey Nun’s Hospital, Edmonton (Dan Stollery) • University of Wisconsin (Ken Kudsk) • Oregon Health Sciences University (Robert Martindale)
TOP UP Teamwork Site Investigator Regulatory Inclusion/exclusion criteria ICU infection adjudication SAE reporting Nurse Adjust EN + PN hourly Product Reconstitution? Pharmacist Checking allocation Dispensing Logs Dietitian Dosing Calculation Optimizing nutrition Monitoring Adequacy Study Coordinator Regulatory Screening/Randomization Pharmacy communication Data collection Study intervention monitoring Collaboration with SI SAE reporting Protocol Violation reporting
Role of Site Investigator Delegation of Authority Patient EligibilityICU Infection adjudicationSAE identification/assessment Investigator Confirmation
Delegation of Authority Logs “The Investigator should maintain a list of appropriately qualified persons to whom the investigator has delegated significant trial-related duties (ICH section 4.1.5)” Completed Log to be sent to CERU before start of trial Imp Manual p 11,12
Inclusion Criteria Imp Manual p 13, CRFs If using estimated weight/height, you may add a buffer of 1 for BMI after rounding 1) Mechanically ventilated adult patients (≥18 years old) 2) Expected to remain mechanically ventilated for more than 48 hours 3) On enteral nutrition or expected to initiate enteral nutrition within 7 days from ICU admission 4) BMI < 25 or >35 based on pre-ICU actual or estimated dry weight
Exclusion Criteria Imp Manual p 14, CRFs • >72 hours from admission to ICU to time of consent (your ICU) • Not expected to survive an additional 48 hours from screening evaluation • Lack of commitment to full, aggressive care (anticipated withholding or withdrawing treatments in the first week but isolated DNR acceptable) • Patients already receiving PN on admission to ICU (does NOT refer to those that received PN in hospital prior to this acute episode of illness)
Imp Manual p 14, CRFs Exclusion Criteria 5. Patients with diabetic ketoacidosis or non ketotic hyperosmolar coma 6. Pregnant or lactating patients 7. Patients with clinical fulminant hepatic failure (see definition) 8. Patients with Cirrhosis Child’s Class C Liver Disease (except those on a transplant list or transplantable) 9. Dedicated port of central line not available 10. Known allergy to study nutrients (soy, egg or olive products) • Enrolment in another industry sponsored ICU intervention study (co- enrollment in academic studies will be considered on a case by case basis)
Eligibility confirmation Document in the medical chart or Sign worksheet by MD and keep as source Prompted at time of Pre randomization Refer to Consent Training Slides
Infection AdjudicationSite Investigator to make determination of a newly acquired infection based on antibiotic and microbiology data
Infection Adjudication CRS/REDCAP manual p 21-27
Suspicion of ICU Infection: Antibiotics Is this antibiotic prescribed for prophylaxis? Is this a substitute for an antibiotic previously ordered for an infection that occurred within 72 hrs of admission to ICU? CRFs p 40, 41 NO to both YES to either Clinical Suspicion of Infection Need adjudication by Site Investigator/MD Delegate No adjudication needed
Suspicion of ICU Infection: Microbiology Is this organism a manifestation of an infection that occurred within the first 72 hrs of admission? CRFs p 42, 43 NO YES Clinical Suspicion of Infection Need adjudication by Site Investigator/MD Delegate Indicate if: Relapse/Recurrent OR Persistent infection No adjudication needed
CRS/REDCAP Manual p 24 Infection Adjudication: REDCAP • This is a newly acquired infection • This is NOT a newly acquired infection • This is a previously adjudicated infection
Infection Adjudication Site Investigator will need: • Access to view the Infection Adjudication table on REDCAP (Research Coordinator to show this) • Appendix 9 Categories of Infection • Appendix 10 Definitions of No Newly Acquired Infection • Medical Chart Refer to CRS/REDCAP Manual pages 21-27 for step by step process
SAE Identification Imp Manual p XX-XX An unexpected adverse event is that event that is NOT expected due to the progression of the underlying disease or co-morbid illnesses. Adverse Event must be serious and unexpected to be reported A serious adverse event is any untoward medical occurrence that at any dose, • Results in death • Is life threatening (the subject was at immediate risk of death from the event • Results in persistent or significant disability/incapacity • Requires in patient hospitalization possibly related to the use of the study materials • Prolongs of hospitalization. • Is a congenital anomaly or birth defect • Is an important medical event that may jeopardize the patient and may require medical or surgical intervention to prevent one of the outcomes listed above medically important condition
Imp Manual p X SAE Reporting (to CERU) Must be done on electronic data capture system and faxed to CERU
SAE Reporting to Regulatory Bodies If SAE is related, CERU will report to Regulatory bodies, Sites and Baxter within 7 days (fatal) or 15 days (non fatal)
Investigator Confirmation CRS/REDCAP Manual p 30
Imp Manual p X Study Groups
Dosing Procedures (both groups) Dosing of the intervention will depend upon the energy and protein needs of the patient To be determined by the dietitian/MD
Protein and Calorie needs Protocol, Imp Manual p X Guidelines for Dosing of Protein and Energy Based on BMI • Upon enrolment, the dietitian/MD will: • Calculate prescribed energy and protein intake as per standard practice • 2. Ensure that minimum energy and protein needs are met as follows *Obesity-adjusted Body weight= IBW + [actual weight – IBW] x 0.25, where IBW is ideal body weight (BMI of 25)
Imp Manual p X Prescribed Volume 3. Determine the prescribed volume for EN (or study PN, or EN + study PN) in mls/24 hrs to meet the prescribed energy and protein needs MUST use enteral formula of 1.2 0.2 kcal/ml Meet protein needs over energy needs 4. Determine the hourly rate of EN (or study PN, or EN + study PN) (assume PN = 1 Kcal/ml) Must be done asap after randomization
Other considerations…Propofol Propofol calories to be factored into assessment of caloric needs, only as per discretion of dietitian/MD
Imp Manual p X Enteral Nutrition (both groups) • Enteral Nutrition to start as per usual practice (patient stabilized, NG/Feeding tube in place) • Standard enteral nutrition formula 1.0 to 1.4 kcals/ml • (hypercaloric formulas not allowed) • NO protein supplements (for 7 days) • NO probiotics (for 7 days) • NO glutamine supplements (for 7 days) • Start at 25 ml/hr and increase every 4 hrs as tolerated until goal rate • Discontinue when the feeding tube comes out Refer to Enteral Nutrition Algorithm & Paired Feeding Algorithm appendices C & F
Imp Manual p X Trace Elements and Multivitamins • DO NOT add to the PN solution • If patient does not receive EN and is dependant on PN for >48 hrs, IV supplementation is recommended Suggested guidelines • Standard doses of multivitamins • 5 mg zinc • 1 mg copper • 0.5 mg manganese • 10 mg chromium • 60mcg selenium. • use commercially available trace element solutions doses can be adjusted at discretion of the medical team
Dietitian Determine Energy/protein needs (prescribed Volume) Follow Canadian Clinical Practice Guidelines Assist with data collection Baseline Nutrition Assessment Daily EN monitoring Daily PN monitoring (non study PN)
CRFs p 12-13 Baseline Nutrition
CRFs p 20-21,23 Daily EN Monitoring
CRFs p 22, 24 Daily PN Monitoring (non study PN)
CRFs p 3 Study Days and Data Collection Data MUST be collected according to calendar day as described below Do NOT collect data according to your flow sheet unless it runs from 00:00 to 23:59 (midnight to midnight)