Download
1 / 41
450 likes | 857 Views
WBC Morphology and Cases. Dr. Gilbert’s Lab. OBJECTIVES:. Learn how to identify the types of white blood cells normally present in a differential count. Recognize abnormalities in white blood cell numbers and what they imply.

E N D
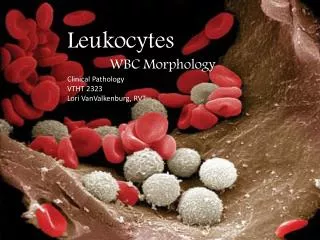
WBC Morphology and Cases Dr. Gilbert’s Lab
OBJECTIVES: • Learn how to identify the types of white blood cells normally present in a differential count. • Recognize abnormalities in white blood cell numbers and what they imply. • Identify changes in white blood cell number and morphology with infection and leukemia.
HOW TO REVIEW A BLOOD SMEAR • First, look under low power to find the area where the cells can be best evaluated, i.e., towards the feathered edge of the smear. Then, look at the slide under medium power to estimate the leukocyte count and to determine whether the white blood cells are of one cell type (abnormal) or whether there are several types of white blood cells present (normal). As you gain experience in looking at blood smears, the medium power is good for picking up immature cells (blasts) when there are only a few of these present. • Next, examine the cells under high power (40X objectives and 100X oil objective). Be sure to wipe the oil from your objective and the slide; otherwise, you will get the oil on your other objectives. Examine the red blood cells, white blood cells, and platelets systematically. In this laboratory session, we are mainly concerned with white blood cell disorders.
CASE 1 • Description: • These normal blood smears show normal red blood cells, white blood cells, and platelets.
Slide 1.1This normal peripheral smear demonstrates a segmented neutrophil and a band neutrophil.
Slide 1.2This normal peripheral smear demonstrates a segmented neutrophil and a lymphocyte.
Slide 1.3This normal peripheral smear demonstrates a monocyte.
Slide 1.4This normal peripheral smear demonstrates an eosinophil and a lymphocyte.
Slide 1.5This normal peripheral smear demonstrates a basophil, a segmented neutrophil, and a lymphocyte.
Identify the following: • Polymorphonuclear leukocytes (PMN's, neutrophils) • Lymphocytes • Monocytes • Eosinophils • Basophils (may be difficult to find in this smear) • A manual white blood cell differential count consists of looking at 100 white cells and enumerating them in the above categories. An automated white blood cell differential count is done by a laboratory instrument that analyzes thousands of white blood cells and categorizes them as a percentage of granulocytes, lymphocytes, and monocytes.
CASE 2 • History: • This 16 year old male came to the emergency room complaining of severe abdominal pain in the right lower quandrant. He had a fever of 101 F. On physical examination, he had a rigid, board-like abdomen and rebound tenderness in the right lower quandrant. There were no other abnormalities.
Slide 2.1This peripheral smear demonstrates increased segmented and band neutrophils.
Laboratory studies: • Urinalysis was within normal limits. A CBC showed Hgb 14.8 g/dl, WBC 20 X 109/L, and platelet count 240 X 109/L.
Questions: • What is the predominant white blood cell present? • What is the name for this type of leukocyte reaction? • What do you think is the diagnosis in this case?
CASE 2: Neutrophilic Leukemoid Reaction • What is the predominant white blood cell present? The majority of white blood cells present here are polymorphonuclear leukocytes, and notice that, at low power, the white blood cell count is higher than in a normal smear. In addition to the PMN's, a small but increased number of band forms are seen. Other cells present are lymphocytes and monocytes, but these are not increased. However, the platelets are moderately increased in number. • What is the name for this type of leukocyte reaction? The name of this reaction is known as a neutrophilic leukemoid reaction. • What do you think is the diagnosis in this case? The diagnosis in this case is acute appendicitis (most, but not all, cases of acute appendicitis are accompanied by peripheral neutrophilia).
CASE 3 • History: • This 15 year old female was sent home from summer camp because of weakness, lassitude, and sore throat. As her family physician, you found that on physical examination she had an inflamed pharynx, enlarged tonsils, several enlarged and slightly tender lymph nodes in the neck, a palpable spleen, and a tender palpable liver edge.
Slide 3.1This peripheral smear demonstrates atypical lymphocytes.
Laboratory studies: • CBC showed Hgb 14.9 g/dl, WBC 12.5 X 109/L, and platelet count 282 X 109/L
Questions: • What is the predominant white blood cell type? • What is your diagnosis in this case? • What is the differential diagnosis? • What other laboratory test may be helpful in arriving at a specific diagnosis?
CASE 3: Infectious Mononucleosis with Atypical Lymphocytosis • What is the predominant white blood cell type? The predominant cell is a lymphocyte. There is an absolute lymphocytosis with many atypical lymphocytes (large lymphs with abundant light to deep blue cytoplasm, round to ovoid nuclei with occasional indentation, and many nucleoli). • What is your diagnosis in this case? The diagnosis is infectious mononucleosis. • What is the differential diagnosis? The differential diagnosis includes various viral infections including hepatitis and cytomegalovirus. This process should not be confused with leukemia. • What other laboratory test may be helpful in arriving at a specific diagnosis? A serologic test for infectious mononucleosis would confirm the diagnosis in most cases.
CASE 4 • History: • This 30 year old male had noticed progressive weakness for one month. On physical examination, a few small lymph nodes were palpable in both axillae, and the tip of the spleen was palpable. There was also sternal tenderness present.
Auer rod Slide 4.1This peripheral smear demonstrates myeloblasts with Auer rods.
Laboratory studies: • CBC showed Hgb 10.2 g/dl, WBC 67 X 109/L, and platelet count 36 X 109/L
Questions: • What is the predominant white blood cell type in this case? • Do you see any intracytoplasmic markers which are diagnostic in this case? • What is your diagnosis?
CASE 4: Acute Myelogenous Leukemia • What is the predominant white blood cell type in this case? Most of the WBC's in this peripheral smear are myeloblasts. Except for occasional mature neutrophils, intervening stages of maturing neutrophils are not seen. Some nucleated red blood cells are also present. Platelets are reduced in number and some large forms are seen. • Do you see any intracytoplasmic markers which are diagnostic in this case? A diagnostic marker is the presence of slender red, needle- like bodies in the cytoplasm called Auer rods. • What is your diagnosis? The diagnosis is acute myeloblastic leukemia (AML). Most patients with acute leukemia have a markedly decreased platelet count. A peroxidase or Sudan black stain will identify the blasts as being of granulocytic series.
CASE 5 • History: • This 65 year old male was in good health except for mild hypertension. At his last check-up, a CBC showed a markedly elevated white blood cell count and physical examination revealed several slightly enlarged lymph nodes in the neck and the axillae, and the spleen was palpable.
Slide 5.1This peripheral smear demonstrates increased numbers of small mature lymphocytes.
Laboratory studies: • CBC showed Hgb 12.8 g/dl, WBC 130 X 109/L, and platelet count 330 X 109/L
Questions: • What is the predominant white blood cell type present? • What is the differential diagnosis?
CASE 5: Chronic Lymphocytic Leukemia • What is the predominant white blood cell type present? Most of the white blood cells are small to medium-sized lymphocytes. There are also many smudged lymphocytes present. In addition, one sees some larger lymphocytes with abundant cytoplasm and a prominent nucleolus which are prolymphocytes. • What is the differential diagnosis? The only real diagnostic consideration in this case is chronic lymphocytic leukemia (CLL).
CASE 6 • History: • This 52 year old male had gradually increasing fatigue together with discomfort in the left upper quandrant. Physical examination revealed an easily palpable spleen and liver edge. A few slightly enlarged lymph nodes were palpable in the neck.
Slide 6.1This peripheral smear demonstrates increased numbers of granulocytes, mostly mature forms, as well as increased platelets.
Slide 6.2This peripheral smear demonstrates increased numbers of granulocytes with mature and immature forms.
Laboratory studies: • CBC shows Hgb 13.2 g/dl, WBC 46 X 109/L, and platelet count 754X 109/L
Questions: • What type of white blood cells are present? • What is the differential diagnosis and how would you resolve it? • What is the diagnosis in this case?
CASE 6: Chronic Myelogenous Leukemia • What type of white blood cells are present? The white blood cell count is moderately elevated, with a wide spectrum of granulocytes at various stages of maturation (rare blasts and promyelocytes, myelocytes, metamyelocytes, bands, and PMN's). In addition, there is an increase in eosinophils and basophils (which would help to rule out a leukemoid reaction as a cause for the WBC elevation). Platelets are moderately increased in number and some large forms are seen. • What is the differential diagnosis and how would you resolve it? The differential diagnosis is leukemoid reaction versus chronic granulocytic leukemia. The increase in eosinophils and basophils suggests leukemia. A leukocyte alkaline phosphatase (LAP) score would also help (high with leukemoid reaction, low with myelogenous leukemia). A Philadelphia chromosome identified by cytogenetic studies on an bone marrow aspirate would help to confirm CML. • What is the diagnosis in this case? The diagnosis is chronic granulocytic (myelogenous) leukemia (CML).
CASE 7 • History: • A 5 year old boy has been too tired to play with his friends for two months. His mother is also worried that, whenever he falls or bumps into anything, a big bruise forms. For the past two days he has had a high fever.
Slide 7.1This peripheral smear demonstrates increased numbers of immature lymphocytes.
Laboratory studies: • CBC shows Hgb 9.8, Hct 28.2, MCV 95, platelet count 74,000, and WBC count 2,300 with differential count 23 segs, 15 bands, 12 monos, 44 lymphs, 5 eos, and 1 baso. A bone marrow biopsy shows replacement by primitive cells that have large nuclei with delicate chromatin and indistinct nucleoli. There is scanty cytoplasm with no granules and no Auer rods. These cells mark for CD10 (CALLA) antigen.
Questions: • What type of white blood cells are present? • What is the most likely diagnosis? • What is the most likely outcome of this child's disease with standard therapy? • What other test could be helpful in distinguishing the nature of the cells in this case?
CASE 7: Acute Lymphocytic Leukemia • What type of white blood cells are present? The white blood cells present are predominantly lymphoblasts. • What is the most likely diagnosis? The most likely diagnosis is acute lymphocytic leukemia (ALL). • What is the most likely outcome of this child's disease with standard therapy? The most likely outcome of this child's disease with standard therapy is good--a >90% chance for complete remission following chemotherapy. • What other test could be helpful in distinguishing the nature of the cells in this case? A TDT (terminal deoxyribonucleotidyl transferase) test is positive in cases of lymphoid leukemias.