Download
1 / 36
370 likes | 406 Views
Learn about renal colic, its symptoms, diagnosis, and treatment options including conservative management, MET, and interventions like ureteroscopy. Understand the role of imaging, analgesia, and admission criteria.

E N D
Renal Colic Local Management Dan Aleksandrov 2019
Kidney Stones Non infection stones Infection stones Genetic aetiology Drug stones
Obstruction location Kidney Calyx PUJ Pelvic brim the iliac vessels arches VUJ
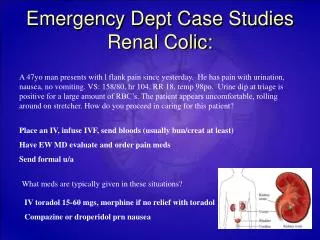
Urinary Tract Stones Renal stones - vague flank pain, haematuria or UTI Ureteric stones - severe ureteric colic, sepsis - Asymptomatic Bladder stones - LUTS, UTI’s , asymptomatic
Renal colic definition Hippocrates- An acute pain is felt in the kidney , the loin, the flank and the testis of the affected side. The patient passes urine frequently , gradually the urine is suppressed. With urine sand is passed.
Symptoms Pain Nausea and vomiting Visible haematuria ⅓ , non visible haematuria Fever Anuria Asymptomatic
Ureteric colic Sudden onset Colicky Rolling around in agony Radiating to the groin and the genitalia Penile pain - ? intramural part of the ureter Even with the above symptoms 50% don’t have stone ( Smith RC 1996, Thompson JM 2001 : CT IVU)
Examination Full external examination Check for masses Check the observation Urine output !
Aetiology Urological - Clot colic(RCC) Tumour colic PUJ obstruction Papillary necrosis Infection Testicular torsion
Aetiology Non-urological Vascular AAA Medical - pneumonia ,MI, malaria Gynae- ovarian cyst torsion, ectopic GI- appendicitis, diverticulitis, peptic ulcer, bowel obstr. Neurological- spinal cord pathology
Aetiology Ureteric stone is rarely life threatening but other causes of pain might be!!!
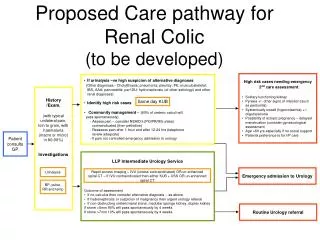
Investigations Bloods Urine dip Pregnancy test Blood cultures if pyrexia ABG Imaging - CTKUB, USS renal, XR KUB, MRU
Renal USS Good to check for hydronephrosis No radiation Kidney and VUJ stones > 5mm 96% sensitivity and 100% specificity Other locations - sensitivity 78%, specificity 31%
CT KUB ( Spiral Non- contrast CT) Golden standard Sensitivity - 97%, detects 1 mm calculi Low dose if BMI<30 Shows complications and other pathologies No contrast required Check stone density and location(stone to skin) Radiation! No renal function evaluation.
High Risk Group Solitary kidney Fever Doubtful diagnosis Bilateral obstruction DM Low immunity Renal impairment
Analgesia NSAIDS- 1st choice Less ureterospasm and eGFR leading to less renal capsular pressure. Less inflammation Avoid when eGFR is low, peptic ulcer ,asthma Opioids- complications!
Indication for Admission Intractable pain or vomiting Obstruction with infection Urinary extravasation Renal impairment Relative indications -high grade obstruction, solitary kidney, intrinsic renal disease, stone size, other.
Spontaneous Passage Rate Metanalysis - 328 patients <10mm 95% of stones up to 4mm passed within 40 days. <5mm - 66% >5mm - 47% <2mm - 31 days 2-4mm - 40 days >4-6mm- 39 days
Conservative management Discharge with review in 2-3 weeks Analgesia and good hydration Strain urine and save the stone for analysis To return in case of fever, chills, intractable pain or vomiting
Observation for Ureteric Stones Well controlled pain No evidence for sepsis Stable renal function Follow up closely
MET ( Medical Expulsive Therapy) Alpha blockers improve the stone passage 10.5 vs 6 days 54% vs 79% Off- license?
Interventions Stent insertion Primary ureteroscopy Nephrostomy ESWL PCNL Open/laparoscopic procedures
Important ! Exclude other causes of pain Pain control CT KUB - golden standard Selective criteria for admission Discuss the treatment options.
Obstructed Infected Kidney Urological emergency! Antibiotics Nephrostomy or Stent (system decompression ) Urine and blood cultures Hydration ITU
Lithotripter Combination ultrasonic and pneumatic urological lithotripter Four sizes of rigid pneumatic probes for use in the kidney, ureter and bladder Designed for use through flexible endoscopes
Lithotripter Available (Theatre 1) Consultant use only Staff training……. Assistants
Primary ureteroscopy and LASER stone fragmentation Removal/fragmentation of stone(s) in the ureter or kidney Rigid or flexible scope
Primary ureteroscopy and LASER stone fragmentation PCH Theatre 1 - NOT Available Consultant only ?! Staff training Assistant
Baskets The Stone Retrieval Basket is intended to be used during urological procedures to endoscopically grasp, manipulate and remove calculi and other foreign objects.
Guide wires Guidewiresare engineered to ensure rapid access, easy advancement, smooth tracking, and maximum manoeuvrability. They help maintain precise control at every step of the procedure.
JJ ureteric STENTS Description: Ureteric stent, is a thin tube inserted into the ureter to prevent or treat obstruction of the urine flow from the kidney. The length of the stents used in adult patients varies between 24 and 30 cm
JJ ureteric STENTS Description Indication Ureteral obstruction due to nephrolithiasis, tumour, or retroperitoneal fibrosis can be uncomplicated, or complicated by urinary tract infection, renal insufficiency, or renal failure
JJ ureteric STENTS Description Indication Variations: Length Size Preference
JJ ureteric STENTS Description Indication Variations Complications: Side effects BAUS consent!
JJ ureteric STENTS Description Indication Variations Complications Follow up/removal: eTCI request
References *Urology Emergency course presentation Mr S. Hayek Addenbrooke’s Hospital *BAUS website