Download
1 / 70
790 likes | 1.83k Views
DISORDERS OF THE THYROID AND PARATHYROID GLANDS. HYPERTHYROIDISM. ETIOLOGY/PATHOPHYSIOLOGY Also called Graves’ disease, or exophthalmic goiter, or thyrotoxicosis DUE TO : Overproduction of the thyroid hormones T3 and T4 Exaggeration of metabolic processes. HYPERTHYROIDISM.

E N D
HYPERTHYROIDISM • ETIOLOGY/PATHOPHYSIOLOGY • Also called Graves’ disease, or exophthalmic goiter, or thyrotoxicosis • DUE TO: Overproduction of the thyroid hormones T3 and T4 Exaggeration of metabolic processes
HYPERTHYROIDISM • ETIOLOGY/PATHOPHYSIOLOGY cont. • Exact cause unknown • Possible genetic factors with precipitive factors of: • Infection, ↓ iodine, or extreme physical or emotional stress • Affects females more than males • May occur during adolesence or pregnancy
HYPERTHYROIDISM • CLINICAL MANIFESTATIONS: • Edema of the anterior portion of the neck • Exophthalmos (bulging eyeballs) • SUBJECTIVE ASSESSMENT : Pt. C/o: • Inability to concentrate; memory loss • Dysphagia • Hoarseness • Increased appetite • Weight loss, insomnia • Nervousness, jittery, excitable
HYPERTHROIDISM • CLINICAL MANIFESTATIONS • OBJECTIVE ASSESSMENT • Tachycardia; hypertension; bruit over thyroid • Warm, flushed skin • Fine hair • Amenorrhea • Elevated temperature/heat intolerance • Diaphoresis • Hand tremors, clumsiness • Hyperactivity for some
HYPERTHYROIDISM • DIAGNOSTIC TESTS • Confirmed by: • ↓ TSH and ↑ Free T4 • RAIU – radioactive iodine uptake – uptake of 35-95% of the drug
HYPERTHYROIDISM • MEDICAL MANAGEMENT • Medications – Block production of thyroid hormone • Propylthiouracil / PTU • Methimazole/ Tapazole • Meds reduce symptoms in 6-8 wks.
HYPERTHYROIDISM • MEDICAL MANAGEMENT • Medication may be followed by: • Radioactive iodine/ ablation therapy • Destroys some of the hypertrophied thyroid tissue • Low dose – no “radiation” precautions needed
HYPERTHYROIDISM • MEDICAL MANAGEMENT cont. • Radioactive iodine/ Ablation therapy cont. • Outcome: in most pts. hypothyroidism treat with Levothyroxine • Adequate medical supervision follow up is important!
HYPERTHYROIDISM • MEDICAL MANAGEMENT cont. • Surgery: for pts. who cannot tolerate antithyroid drugs; are not good candidates for radiation tx.; have a poss. malignancy; or have large goiters causing tracheal compression • Most common surgery: Subtotal Thyroidectomy • Removal of 5/6ths of the thyroid gland • If too much thyroid tissue is removed gland will not regenerate hypothyroidism
HYPERTHYROIDISM • MEDICAL MANAGEMENT cont. • Surgery: usually delayed until pt in a normal thyroid state d/t the risk of bleeding during surgery and thyroid crisis (thyroid storm) post op.
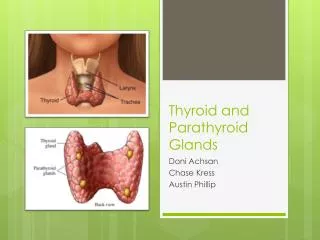
HYPERTHYROIDISM • NURSING ASSESSMENT AND INTERVENTIONS: • Post-operative Subtotal Thyroidectomy • Assess for s/sx internal or external bleeding • Assess for tetany: • Chovstek’s Sign: is + when abnormal spasm of facial muscles occurs when elicited by light tapping on facial nerve in the pt. with low calcium • Trousseau’s Sign: is + if there is carpal spasm in the hypocalcemic and hypomagnesemia pt. When BP cuff inflated above pt. normal systolic pressure and held there for 3 min.
HYPERTHYROIDISM • NURSING ASSESSMENT AND INTERVENTIONS: • Post-op Subtotal Thyroidectomy (cont.) • Assess for Thyroid Crisis/Storm • May occur as a result of manipulation of the thyroid gland during surgery releasing large amts of thyroid hormone bloodstream • Occurs within the first 12 hrs. • S/SX: exaggerated s/sx of hyperthyroidism + n/v, severe tachycardia, severe HTN, severe hyperthermia (106F+), extreme restlessness, dysrhythmias, delirium, heart failure death
HYPERTHYROIDISM • Thyroid Storm cont.: • DIAGNOSTIC TESTS • ↑FT4, ↓TSH • MEDICAL MANAGEMENT goals during thyroid storm: • 1. induce a normal thyroid state • 2. prevent cardio-vascular collapse • 3. prevent ↑ hyperthermia
HYPERTHYROIDISM • NURSING ASSESSMENT AND INTERVENTIONS: • Post-op Subtotal Thyroidectomy (cont.) • Voice rest x48 hrs – provide communication tool • Voice checks – q 2-4 hrs. “ahh”; note hoarseness or other changes • Bed – semifowler’s position; pillow support for head and shoulders
HYPERTHYROIDISM • NURSING ASSESSMENT AND INTERVENTIONS: • Post-op Subtotal Thyroidectomy (cont.) • Avoid hyperextension of neck; support head during position change • Reinforce DB exercises; check with MD re: coughing • Tracheotomy tray at bedside and suction • Cool mist humidifier prn • Nutrition care – watch for dysphagia
HYPERTHYROIDISM • NURSING DIAGNOSES: • Pre-op • Risk for hyperthermia, related to increased metabolism • Imbalanced nutrition:less than body requirements r/t increased metabolism • Post-op • Impaired swallowing, r/t edema • Ineffective breathing,risk for, r/t post-op edema and pain
HYPERTHYROIDISM • PATIENT EDUCATION • Post op: • follow up with medical supervision • Thyroid function tests • Care incision site • Diet: high calorie, CHO’s , and protein • PROGNOSIS: nml life with appropriate medical or surgical tx. • Expophthalmos may remain to lesser degree
HYPOTHYROIDISM • Etiology/pathophysiology • Due to insufficient secretion of thyroid hormones • Decreasedhormones cause slowing of all metabolic processes • R/T Failure of thyroid or insufficient secretion of thyroid-stimulating hormone from pituitary gland
HYPOTHYROIDISM • Myxedema refers to severe hypothyroidismin adults • Will see edema in hand’s face, feet, and periorbital tissues • Cretinism – congenital hypothyroidism
HYPOTHYROIDISM • Clinical Manifestations: • Because all metabolism processes slow • Hypothermia; intolerance to cold • Weight gain • ASHD/CAD ↓exercise tolerance + dyspnea on exertion
HYPOTHYROIDISM • SUBJECTIVE ASSESSMENT: • Mental and emotional assessment may include: • Depression; paranoia • Impaired memory; slow thought process • Hearing/speech impairment • Lethargic, forgetful, irritable • Anorexia • Constipation • Cold intolerance • Decreased libido; reproductive difficulties
HYPOTHYROIDISM • OBJECTIVE ASSESSMENT • Menstrual irregularities • Thin hair, falls out • Skin thick and dry • Enlarged facial appearance • Low, hoarse voice • Bradycardia • Hypotension • Weakness, clumsiness, ataxia
HYPOTHYROIDISM • Diagnostic tests : TSH, T3, T4, FT4 (low levels of these are the underlying stimuli for TSH) • For hypothyroidism: expect ↑TSH (compensatory); ↓T3, T4, and FT4
HYPTHYROIDISM • MEDICAL MANAGEMENT • Medications: replacement therapy; titration needed • Synthroid • Levothyroid • Proloid • Cytomel • Symptomatic treatment
HYPOTHYROIDISM • NURSING INTERVENTION/PT. TEACHING: • For the hospitalized pt. with severe hypothyroidism focus on symptom relief • Watch for s/sx hyperthyroidism while adjusting doses of replacement medication • Watch for chest pain or dyspnea • Keep room 70-74⁰F • Avoid the pt. getting chilled • BM monitor/protocol
HYPOTHYROIDISM • NURSING INTERVENTIONS/PT. TEACHING cont. • Diet : ↑protein, fiber, fluid ↓ calories Adequate iodine intake • Instruct pt. to take med daily and not to stop without consulting his MD • Instruct pt./family – to anticipate clearing of mental slowness as pt. adjusts to dose of med
HYPOTHYROIDISM • NURSING DIAGNOSES: • Decreased cardiac output r/t decreased metabolism • Constipation r/t decreased peristalsis • Risk for noncompliance r/t therapy • Risk for disturbed body image, r/t altered physical appearance (goiter)
HYPOTHYROIDISM • PROGNOSIS: Pt. will do well with medication and medical supervision. • In children, if the T4 replacement begins before the epiphyseal fusion, chance for normal growth is greatly improved
SIMPLE (COLLOID) GOITER • ETIOLOGY/PATHOPHYSIOLOGY • Enlarged thyroid due to low iodine levels or the gland’s inability to use the iodine properly • Enlargement is caused by the accumulation of colloid in the thyroid follicles • When blood level of T3 is too low to signal the pituitary gland to reduce TSH secretion, the thyroid gland responds by increased formation of thyroid globulin (colloid) accumulates in the thyroid follicles gland enlargement • Usually caused by insufficient dietary intake of iodine overgrowth of thyroid tissue
SIMPLE (COLLOID) GOITER • CLINICAL MANIFESTATIONS/ASSESSMENT • Assessment based on physical manifestations: • SUBJECTIVE ASSESSMENT: • Enlargement of the thyroid gland • Pt. emotional response to the enlargement • Interview to determine pt. need for medication, diet, and medical follow up • May c/o: Dysphagia, Hoarseness. Dyspnea
SIMPLE (COLLOID) GOITER • CLINICAL MANIFESTATIONS/assessment • OBJECTIVE DATA: • Assess increase of goiter • Voice changes • Adequate food/fluid intake • MEDICAL MANAGEMENT • Potassium iodide • Diet high in iodine • Surgery—thyroidectomy
SIMPLE (COLLOID) GOITER • NURSING INTERVENTIONS/GOALS • Post Thyroidectomy: prevent complications such as bleeding, tetany, and thyroid crisis • Interventions: (discussed previously) • NSG. DIAGNOSES • Risk for non-compliance with therapeutic regimen • Risk for disturbed body image r/t physical appearance
Figure 51-10 Simple goiter.
Thyroid Cancer • ETIOLOGY/PATHOPHYSIOLOGY • Malignancy of thyroid tissue; rare • About 75% are papillary well-differentiated adeno carcinoma- grows slowly, usually contained, doesn’t spread beyond adjacent lymph nodes; cure rates are excellent. • CLINICAL MANIFESTATIONS • Firm, fixed, small, rounded mass or nodule on thyroid
Thyroid Cancer • Assessment • SUBJECTIVE ASSESSMENT • Pt. coping method and support system • Pt. understanding of importance of medical follow up • OBJECTIVE ASSESSMENT • Progressive enlargement of tumor area • Response to 131I tx. • Skin care post radiation
Thyroid Cancer • DIAGNOSTIC TESTS: • Thyroid scan • Thyroid function tests • Needle bx. • MEDICAL MANAGEMENT • Total thyroidectomy • Thyroid hormone replacement • If metastasis is present: radical neck dissection; radiation, chemotherapy, and radioactive iodine
Thyroid Cancer • NURSING INTERVENTIONS/Pt. TEACHING • Per thyroidectomy (previously discusses) • Post op: • Risk for respiratory distress • Risk for laryngeal damage • Bleeding • S/sx hypothyroidism
Thyroid Cancer • NURSING DX. • Anxiety r/t situational crisis • Ineffective coping r/t personal vulnerability in a crisis • Pt. Teaching: • Proper medical follow up • Monitor thyroid replacement therapy • Proper care of surgical incision
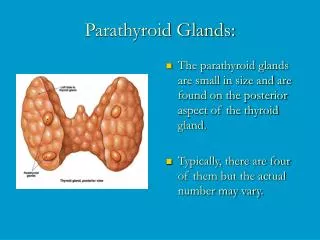
HYPERPARATHYROIDISM • ETIOLOGY/PATHOPHYSIOLOGY • Overactivity of the parathyroid glands, with increased production of parathyroid hormone (PTH) • Hypertrophy of one or more of the parathyroid glands (usually in the form of an adenoma) • Also from: CRF, Pyelonephritis, glomerulonephritis
HYPERPARATHYROIDISM • CLINICAL MANIFESTATIONS • Hypercalcemia – primary clinical manifestation • Calcium leaves the bone serum calcium increases • Bones become demineralized formation of renal calculi, pathological fx. • Skeletal pain; pain on weight-bearing