Download
1 / 49
570 likes | 1.3k Views
DISORDERS OF THYROID AND PARATHYROID GLAND AND THEIR MANAGEMENT Prof. Dr. S. N. Ojha M.D. (Ayu.) Phd. Dean & Superintendent Dr. D. Y. Patil College of Ayurveda & Research Centre Pimpri, Pune. What is Thyroid?

E N D
DISORDERS OF THYROID AND PARATHYROID GLAND AND THEIR MANAGEMENT Prof. Dr. S. N. Ojha M.D. (Ayu.) Phd. Dean & Superintendent Dr. D. Y. Patil College of Ayurveda & Research Centre Pimpri, Pune.
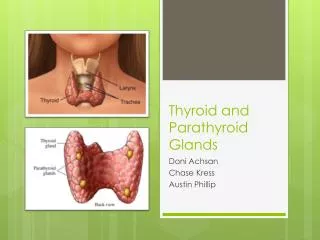
What is Thyroid? The thyroid is a small gland, shaped like a butterfly, located in the lower part of your neck. The main hormones released by the thyroid are triiodothyronine, (T3) & thyroxine, (T4) What Diseases and Conditions Affect the Thyroid? Hypothyroidism – An underactive thyroid. Hyperthyroidism – an overactive thyroid. Goiter – An enlarged thyroid. Thyroid Nodules – Lumps in the thyroid gland. Thyroid Cancer – Malignant thyroid nodules or tissue. Thyroiditis – Inflammation of the thyroid.
Hyperthyroidism : Hyperthyroidism is a condition where the thyroid gland – the master gland of metabolism – is overactive. Causes of Hyperthyroidism • Graves’ disease. • Thyroiditis • Autoimmune condition Hashimoto’s disease, a temporary hyperthyroidism that affects women
Risk of Graves’ Disease / Hyperthyroidism • Female gender • Personal and family history of thyroid problems, autoimmune disease, or endocrine disease • Age 20 and 40 • Pregnancy – During pregnancy and the year after childbirth • Current or former smoker
Excessive intake of thyroid hormone • Exposure to or excess of iodine/iodine drugs • Certain medical treatments • Trauma to the thyroid • Recently experienced major life stress • Holistic and nutritional factors
Common symptoms • Goiter, thyroid enlargement, neck sensations • Weight and appetite changes • Pregnancy-related problems • Feeling warm all the time, sweating, thirst, fever • Heart and blood pressure changes, fast heart rate, abnormal heart rhythms • Bowel problems, diarrhea • Fatigue, exhaustion • Muscle and join pain and fatigue
Skin changes, blister-like bumps on the forehead and face, hives, itching, vitiligo. • Skin patches on the shins and legs (Graves’ dermopathy / pretibial myxedema) • Hair loss and other hair changes. • Finger/nail changes, including swollen, wider fingertips and separation of nail bed from skin. • Eye problems, including bulging, dryness, pain, redness, puffiness
Thinking/cognition problems, including difficult concentrating or making decisions, memory problems, and racing thoughts. • Changes to mood and feelings, including depression, mood swings, uncontrollable anger, irrational anger. • Panic and anxiety, panic attacks • Fast reflexes, startling, tremors • Insomnia
Diagnosing Graves’ Disease Clinical Exam. • Feel (also known as “palpating”) neck • Palpate for what’s known as “thrill” • Listen for “bruit” during palpation • Test reflexes-hyper responsive reflexes can be a sign of hyperthyroidism • Heart rate, rhythm & blood pressure • Measure weight • Measure body temperature
Examine face and neck area • Examine skin for some possible signs of hyperthyroidism • General quantity and quality of hair • Tremors • Nails and hands for thyroid signs • Evaluate legs • Examine eyes
Test results that confirm hyperthyroidism include: TSH Test – usually below normal, to undetectable T4/Free T4 Test – Normal to High T3/Free T3 Test – Normal to High Radioactive Iodine Update (RAI-U) Test Elevated Thyroid Receptor Antibodies (TRAb) / Thyroid-Stimulating Immunoglobulin (TSI).
Hyperthyroidism – can be treated with three different approaches: • Drug treatment with antithyroid drugs • Ablation of the thyroid gland with Radioactive Iodine (RAI) • Surgery to remove all or part of the thyroid. Antithyroid Drug Treatment • Methimazole - Carbimazole • Propylthiouracil Radioactive Iodine Treatment • Radioiodine ablation • Radioactive iodine ablation • Thyroid ablation • Ablation therapy • Chemical thyroidectomy • Chemical surgery • Radioactive cocktail
Ayurvedic Treatment • Kanchanar Guggulu • Aarogyavardhini Rasa • Sootshekhar Rasa • Dasha moolarishta
Hypothyroidism : When the thyroid gland is underactive, improperly formed at birth, surgically removed all or in part, or becomes incapable of producing enough thyroid hormone, a person is said to the hypothyroid.
Causes • Iodine deficiency • Hashimoto’s thyroiditis • Lack of the thyroid gland • Deficiency of hormones from either the hypothalamus or the pituitary. • Postpartum thyroiditis • Sporadic inheritance, sometimes autosomal recessive • Wolff-Chaikoff effect • Lithium-based mood stabilizers
Symptoms Early symptoms • Poor muscle tone • Fatigue • Cold intolerance • Depression • Muscle cramps and joint pain • Arthritis • Goiter • Thin, brittle fingernails • Thin, brittle hair • Paleness • Dry, itchy skin • Weight gain and water retention • Bradycardia (low heart rate: less than sixty beats per minute) • Constipation
Late symptoms • Slow speech and a hoarse, breaking voice. • Dry puffy skin, especially on the face • Thinning of the outer third of the eyebrows. (sign of Hertoghe) • Abnormal menstrual cycles • Low basal body temperature Less common symptoms • Migraine headache • Impaired memory • Anxiety / panic attacks • Urticaria
Impaired cognitive function and inattentiveness • A slow heart rate with ECG changes including low voltage signals. • Reactive (or post-prandial) hypoglycemia • Pericardial effusions may occur. • Sluggish reflexes • Hair loss • Early greying of the hair • Anemia caused by impaired hemoglobin synthesis • Difficulty swallowing • Shortness of breath with a shallow and slow respiratory pattern
Hypercapnia & hypoxia • Increased sleep • Osteopenia or Osteoporosis • Irritability and mood instability • Yellowing of the skin • Impaired renal function • Thin, fragile or absent cuticles • Elevated serum cholesterol • Acute psychosis • Decreased libido
Decreased sense of taste and smell • Puffy face, hands and feet • Premature wrinkling on the face Pediatric • Short stature • Mental retardation • Short neck • Delayed development
Severity • Cardiovascular & psychiatric • Myxedema Diagnostic testing • Free triiodothyronine (fT3) • Free levothyroxine (fT4) • Total T3 • Total T4 • 24 hour urine free T3 • antithyroid antibodies • Serum cholesterol • Prolactin • Testing for anemia, including ferritin • Basal body temperature
Treatment • Levorotatory forms of thyroxin (L-T4) • Different treatment protocols in thyroid replacement therapy: • T4 Only • T4 and T3 in Combination • Desiccated Thyroid Extract
Ayurvedic Treatment • Laxmivilas Rasa • Punarnavadi Mandur • Agnitundi Vati • Ashwagandharishta • Amrtarishta • Shatavari • Chitrak • Chatusparni
Autoimmune Thyroid Disease In the case of autoimune thyroid disease, antibodies either gradually destroy the thyroid, or make it overactive. • Goiter/Thyroid Nodules When the thyroid become enlarged, this is known as a goiter. • Thyroid Cancer • Thyroiditis When the thyroid become inflamed, due to bacterial or viral illness, this is known as thyroiditis Treatments – Surgery, Thyroid drugs
Parathyroid gland • The parathyroid glands are small endocrine gland in the neck that produces parathyroid hormone. • Most people have four parathyroid glands, but some people have six or even eight
Hypoparathyroidism It is decreased function of parathyroid glands, leading to decreased levels of parathyroid hormone (PTH).
Causes • Removal of the parathyroid glands in thyroid surgery (thyroidectomy) • Autoimmune. • Hemochromatosis • Chromosome 22q11 microdeletion syndrome (other names: DiGeorge syndrome Schprintzen syndrome, velocardiofacial syndrome). • Magnesium deficiency • DiGeorge syndrome, absence of the parathyroid glands at birth. • Idiopathic, occasionally familial
Signs and Symptoms • Tingling lips, fingers, and toes • Muscle cramps • Pain in the face, legs, and feet • Abdominal pain • Dry hair • Brittle nails • Dry, scaly skin • Cataracts • Weakened tooth enamel (in children) • Muscle spasms called tetany • Convulsions (seizures)
Additional symptoms • Painful menstruation • Hand or foot spasms • Decreased consciousness • Delayed or absent tooth formation Diagnosis • Measurement of calcium • Serum albumin • PTH in blood. • E.C.G.
Differential diagnoses are: • Pseudohypoparathyroidism • Pseudopseudohypoparathyroidism • Vitamin D deficiency or hereditary insensitivity to this vitamin (X-linked dominant). • Malabsorption • Kidney disease • Medication: Steroids, diuretics, some antiepileptics.
Treatment 1. Intravenous calcium Long-term treatment • Calcium and Vitamin D 3 • Teriparatide Possible Complications • Tetany can lead to a blocked airway • Stunted growth, malformed teeth, slow mental development • Overtreatment with vitamin D and calcium can cause hypercalcemia
Pseudohypoparathyroidism Pseudohypoparathyroidism is a condition caused by resistance to the parathyroid hormone. Patients have a low serum calcium and high phosphate, but the parathyroid hormone level (PTH) is appropriately high.
Types • Type 1 a pseudohypoparathyroidism • Type 1 b pseudohypoparathyroidism lacks the physical appearance of type 1 a biochemically similar • Type 2 pseudohypoparathyroidism also lacks the physical appearance of type 1 a. Presentation • Features of hypocalcaemia • Including; carpo-pedal spasm, tetany, muscle cramps and seizures. • Type 1 a Pseudohypoparathyroidism is clinically manifest by blunting of fourth and fifth metacarpals, short stature, obesity, developmental delay.
Biochemical Findings • Hypocalcemia • Hyperphosphatemia • Elevated parathyroid hormone
Hypocalcemia • Muscle spasm • Carpopedal spasm • facial grimacing • Layrngeal spasm • Convulsion • Respiratory arrest may occur • Increase intracranial pressure • Irritability • Depression • Psychosis • Arrhythmias • Intestinal cramps • Chvostek’s or Trousseaus Sign
Treatment • Replacement with Vit. D or Calcitriol • High oral calcium intake • Thiazide diuretics Ayurvedic Treatment • Godanti • Praval Panchamruta
Hyperparathyroidism Hyperparathyroidism is overactivity of the parathyroid glands resulting in excess production of parathyroid hormone (PTH) Classification • Primary Hyperparathyroidism It results from a hyper function of the parathyroid glands themselves. There is over secretion of PTH due to adenoma, hyperplasia or rarely, carcinoma of the parathyroid glands.
Secondary hyperparathyroidism Secondary hyperparathyroidism is the reaction of the parathyroid glands to a hypocalcemia caused by something other than a parathyroid pathology, e.g. chronic renal failure. Tertiary Hyperparathyroidism Tertiary hyperparathyroidism is a state of excessive secretion of parathyroid hormone (PTH) after a long period of secondary hyperparathyroidism and resulting in hypercalcemia.
Etiology Primary hyperparathyroidism 1. benign parathyroid adenoma 2. multiple endocrine neoplasia Secondary hyperparathyroidism Due to excessive secretion of parathyroid hormone (PTH) by parathyroid glands in response to hypocalcemia and/or hyperphosphatemia, usually due to chronic renal failure.
Tertiary hyperparathyroidism Caused by long lasting disorders of the calcium feedback control system. Symptoms and signs Asymptomatic hyperparathyroidism Coincidental finding of hypercalcemia
Symptomatic Hyperparathyroidism Most of the symptoms of parathyroid disease are “neurological” weakness and fatigue, depression, aches and pains, decreased appetite, feelings of nausea and vomiting, constipation, polyuria, polydipsia, cognitive impairment, kidney stones and osteoporosis.
Symptoms of hyperparathyroidism can be remembered by the rhyme “moans, groans, stones, bones, and psychiatric overtones” : • “moans” (complaints of not feeling well) • “groans” (abdominal pain, gastroesophageal reflux) • “stones” (kidney) • “bones” (bone pain) • “psychiatric overtones” (lethargy, fatigue, depression, memory problems)
Laboratory tests Serum calcium • In cases of primary, tertiary hyperparathyroidism increased PTH consequently leads to increased serum calcium (hypercalcemia) • In secondary hyperparathyroidism effectiveness of PTH is reduced. Serum phosphorus • Primary hyperparathyroidism levels are abnormally low • Secondary hyperparathyroidism serum phosphorus levels are generally elevated
Alkaline phosphatase Alkaline phosphatese levels are not elevated in all types of hyperparathyroidism Diagnosis • PTH immunoassay • Tertiary hyperparathyroidism has a high PTH and high serum calcium.
Treatment and monitoring • Surgery If surgery is not available, the following should be monitored • Calcium level • Bone density • Check for kidney stones Prevention • Exercise • Vitamin D-Adequate amounts of vitamin D aid in calcium absorption. • Stay hydrated • No smoking
Hypercalcemia Fatigue Depression Mental Confusion Anorexia Nausea Vomiting Constipation Increased urination Cardiac arrythmias
Treatment • Restricted Dietary Calcium • Rehydration • Forced Diuresis • Calcitonin • Anti resorptive agents (bisphosphonates) • Phosphate therapy