Download
1 / 65
680 likes | 1.04k Views
PATHOPHYSIOLOGY OF THE THYROID AND PARATHYROID GLANDS MUDr. Pavel Maruna. Thyroid gland. Physiology Derived from embryonic thyroglossal duct 2 lobes connected by an isthmus 20 g weight The only significant source of T4, ( T3 ... peripheral conversion)

E N D
PATHOPHYSIOLOGY OF THE THYROID AND PARATHYROID GLANDS MUDr. Pavel Maruna
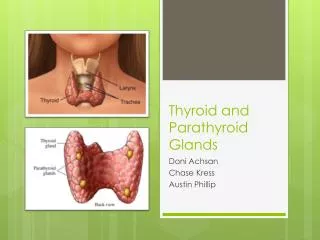
Thyroid gland Physiology Derived from embryonic thyroglossal duct 2 lobes connected by an isthmus 20 g weight The only significant source of T4, ( T3 ... peripheral conversion) T3, T4: 3-, 4- iodine-derivates of tyrosine T3is more potent metabolic factor than T4 Regulation of secretion: TRH - TSH - T4 axis
Thyroid gland Physiology
Examination methods Total T4 (75-170 nmol / L, 80 - 90 g/den), total T3 Free T4 (fT4) 11 - 22 pmol / L, free T3 TSH (0,5-6,5 mU / L) USG, Color Doppler Scintigraphy (131I, 132I, 99mTc) - differ. dg. of hot / cold nodi, ectopic goiter, metastases FNAB (Fine Needle Aspiration Biopsy)
Examination methods Auto-Ab in diagnostics (high specificity) auto-Ab anti-TSH-R binding to different epitops: growth, goiter stimulation ... Graves-Basedow dis. inhibition ... hypothyroid idiopatic myxoedema auto-Ab anti-microsomal = anti-TPO (thyroid peroxidase) ... Hashimoto dis. auto-Ab anti-Tg (thyroglobulin) ... x pathogenetic auto-Ab anti-T3 ... in 40% autoimmmune thyroiditis
Examination methods Color USG: Blood flow
Examination methods 131I scintigraphy: Retrosternal goiter
Examination methods 131I scintigraphy: Thyroid cancer - „cold“ nodule
Examination methods Biopsy (FNAB)
Thyroid gland Pathology Primary disorders (thyroid gland) Secondary disorders (pituitary gland) Receptor disorders
Thyroid gland • Physiological effects: • Essential in fetal development • Heat production • Metabolic activity level (activity of cellular Na/K ATP-ase) • Glucose metabolism (uptake of glucose in GIT) • Cholesterol • Haemopoiesis • Bone formation
Thyroid gland Pathological manifestation 1. Functional hypothyroidism hyperthyroidism 2. Local goiter mechanic syndrome (dyspnoe, dysfagia, vessels) 3. Systemic (non-endocrine) metastases
Thyroid gland Chronic lymfocytic thyroiditis Graves Basedow dis. ... Etiology Normal Hypothyroidism Hyperthyroidism Function Local signs Goiter Mechanic syndrome (dyspnoe, dysfagia, vessel compression
Eufunctional goiter • = Goiter with normal hormonal production, x tumor or inflammation • Usually asymptomatic, event. dysfagia, dyspnoe. • High incidence in last decades x iodine prophylaxis and nutritional status • Etiology • iodine insuf. (endemic goiter) • strumigens in food, drugs (SFA, TBCstatics, Li, resorcinol) • malnutrition • hereditary factors • juvenile goiter (?) • iodine overload (Wolf-Chaikoff effect) - risk of lymphocyte thyroitidis
Thyroid tumors • Carcinoma malignant lymphoma, sarcoma, carcino / sarcoma, adenoma • 2-4x incidence in female • 0,5-1,0 % of all carcinomas, increasing incidence ! • Risk factors: • ion. irradiation (papillary ca) • high TSH (papillary ca, follicular ca) • x relations to jódu
Thyroid tumors • Histological types: • Papillary (60-70 %) - differentiated, low risk, but possible change to anaplastic form • Follicular (15-30 %)- " - • Anaplastic – x differentiated, high malignant • Medullary (from C cells)
Thyroid tumors Clinical course solitary note, slow growth, local pain (invasive growth), dysphagia, dyspnoe lymph node metastases distant metastases (lungs, path. fractures..) 131I scintigraphy: metastases of papillary ca
Thyroid tumors Examination methods USG Gammagraphy – usually „cold node" (x iodine accumulation) FNAB (fine needle aspiration biopsy) - cytology Alternatively: biopsy with Vim-Silverman needle - histology Laboratory Euthyroid status calcitonin, PCT, CEA … medullary ca Tg, anti-Tg … non-medullary ca, using for post-surgical monitoring
Thyroid tumors Prognosis: Relatively good, better in younger patients, differ. forms
Chronic lymphocytis thyreoiditis • Classification (Volfé) • Hashimoto dis. (= with goiter) • autoimmune thyr. in children and adults • chronic fibrotic variant • atrophic variant • primary myxedema • Riedl goiter = rare inflamm. form • Autoimmune dis. (primary defect of TS lymphocytes ?) • auto-Ab anti-Tg • auto-Ab anti-microsomal • … and also other auto-Ab
Chronic lymphocytis thyreoiditis • Etiology: • Genetic dispositions • Family history is positive in 50% ! • HLA-DR5 variant with goiter • HLA-B8, DR3 atrophic variant (see DM type I) • HLA-DR2 lower risk • 30% Turner sy … LT • frequent combination with other autoimmune dis.: • LT in 65% patients with DM type I • POEMS sy • = polyneuropathy, organomegaly, endocrinopathy, • M protein, skin changes • polyglandular sy I, II, III (thyrogastric sy)
Chronic lymphocytis thyreoiditis Pathogenesis: Stimuli - may provoke manifestation of latent LT iodine (cave amiodarone) Li after delivery - LT in 10% females (usually transient, but 25% hypothyroidism) cytokine treatment (IFNα, IL-2, GM-CSF) 10% T4 (TPO inhibition, role of NK Ly dysfunction (T4)
Chronic lymphocytis thyreoiditis Prevalence In non-selected necropsies: 40-45% fem. and 20% males Females 7:1 males, mean age of manifestation 59 yr. Precancerosis? In thyr. lymphoma – prevalence of LT is 80x higher
Graves-Basedow dis. Autoimmmune inflammation Most often cause of thyrotoxicosis Auto-Ab (IgG) anti-TSH R (TRAK, TSI, LATS, LATS protectors) TH Ly The role of provocative stress factors (emotion, fever)
Graves-Basedow dis. Clinical trias: goiter + exophthalmus + tachycardia (oligo- and monosymptomatic forms in old patients)
Hypothyroidism • Etiology • Primary T4, T3, TSH • Secondary T4, T3, TSH • Congenital receptor deficiency - peripheral resistance to the T4 action T4, T3, TSH • 1. Immunopathology (lymphocytic thyroiditis - Hashimoto´s disease) • 2. Iodine deficiency • 3. Subacute thyroiditis
Hypothyroidism • Manifestation: • goiter (hyperplasia of thyroid gland - TSH growth stimulation) • myxedema (forearm, ...) • bradypsychia, lethargy, inability to concentrate • anemia (impaired B12 vit. metabolism) • cardiovascular signs (bradycardia, ventricular dilation) • impaired renal function • neuromuscular system dysfunctions (paresthesia, muscle weakness)
Hypothyroidism Congenital hypothyroidism = cretinism (infants) - mental dysfunction, cyanosis, poor feeding, retardation of bone maturation
Hypothyroidism Laboratory findings T4, free T4, T3 TSH cholesterol macrocytic anemia
Hyperthyroidism Etiology primary T4, T3, TSH secondary T4, T3, TSH (very rare !) Graves disease (diffuse toxic goiter) autoimmune disorder, autoantibody against TSH-receptors Toxic adenoma (carcinoma) of thyroid gland Hashimoto´s thyroiditis (early stage)
Hyperthyroidism Manifestation palpitation, hyperkinesia, excesive sweating thyroid enlargement (goiter) ophthalmopathy upper lid retraction periorbital edema protrusion corneal involvement sight loss loss of muscle mass diarhhea accelerated bone maturation dyspnoe
Hyperthyroidism Laboratory findings T4, free T4, T3 TSH cholesterol
Ca++ PTH Glycoprotein, 115 AA precursor, intracel. storage Proteolytic removal of N-termin. structure 84 AA active hormone Regulation of synthesis / secretion by ↓ plasma Ca2+ Negative feedback regulation PTH receptors on plasma membrane Adenylat cyclase, cAMP action
Ca++ PTH Effects: PTH / Ca2+ regulation Kidney: retention of Ca++ … tubular reabsorption of Ca and Mg Bone: release of Ca++ from bone (osteoclastic x osteoblastic differentiation and action GIT (via vit. D) absorption of Ca++ from the gut
Ca++ PTH Effects:
Ca++ Calcitonin (CT) Product of parafollicular C cells of thyroid gland Peptide, 32 AA, Mv 3,7 kD Precursor - procalcitonin (inflammatory marker) Regulation: Stimulation by ↑ Ca2+ Effects: Ca2+ regulation (low importance in humans) Excess or deficiency has not dramatic clinical manifestation Kidney: release of Ca2+ Bone: uptake of Ca2+
Ca++ Vitamin D Vitamin D3 ... Cholecalciferol Vitamin D2 ... Ergocalciferol Sterol hormones 90 %synthesis in skin 10 % food intake Hydroxylation 25-OH- D3 (liver) 1,25-OH- D3 (kidney)
Ca++ Vitamin D Effects: Increase of plasma Ca2+ and PO4 … conditions for bone mineralization GIT: facilitation of Ca2+ and PO4 absorption Bone: direct effect of ossification of osteoid tissue Skin: trophic effect (x alopecia) Other tissues: immunological effects
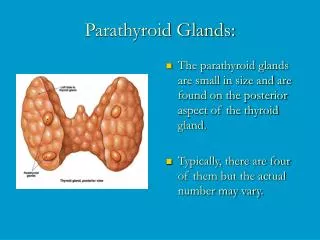
Parathyroid glands 4 bodies near both upper and lower thyroid lobe 0,05-0,30 g 10 - 20 % atypical localization (mediastinum)
Hypoparathyroidism • Etiology: • Postoperative (after TTE … transitory or irreversible) • Idiopathic … Autoimmune destruction of glands, combination with Addison dis. + Hashimoto dis. • Congenital - inactive PTH production • Functional (↓↓Mg2+) … transitory • Pseudohypoparathyroidism • PTH receptor disease in kidneys / or postreceptor dis. • ... Negative feedback … ↑PTH • manifestation: short staue, obesitas, ↓IQ, brachydactylia • Pseudo-pseudo-hypoparathyroidism • ? incomplete manifestation of pseudohypo-PTH
Hypoparathyroidism Acute manifestation: ↓Ca2+ + ↑PO4 → neuromuscular hyperactivity Manifestation depends on actual Ca2+ levels Paresthesia (tingling around mouth, fingers) Hyperventilation (as alarm reaction) → ↓CO2 → alkalosis → Ca2+ binding to proteins Tetany (attact begins with paresthesias … painful spasms of extremities and face … flexion of the wrist and MP joints, extension of IP joints Adrenergic reaction (tachycardia, sweating)