Download
1 / 17
280 likes | 893 Views
Leukemia. Maturation of Myeloid Cells. Dr. Rania Alhady. Leukemia. Definition: Leukemias are a group of disorders characterized by the accumulation of malignant white cells in the bone marrow and blood. • Abnormal cells cause symptoms because of:

E N D
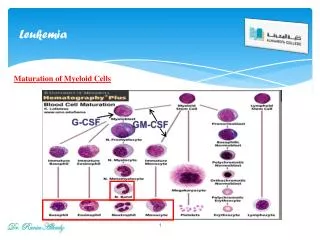
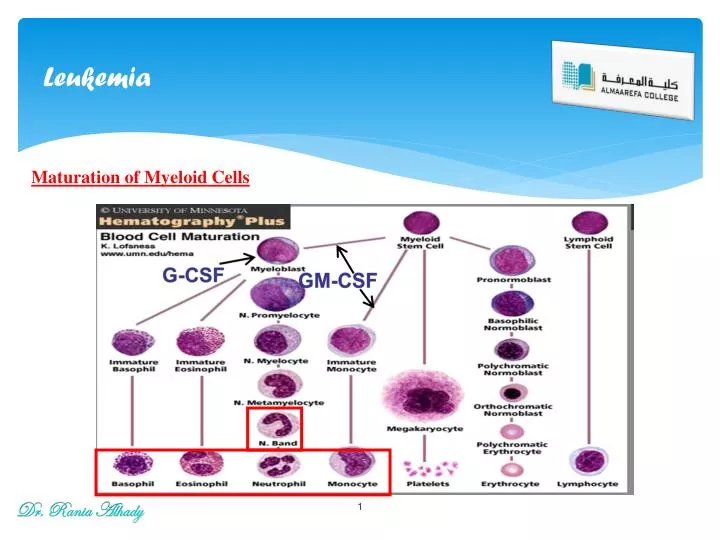
Leukemia Maturation of Myeloid Cells Dr. Rania Alhady
Leukemia Definition: Leukemiasare a group of disorders characterized by the accumulation of malignant white cells in the bone marrow and blood. • Abnormal cells cause symptoms because of: (i) bone marrow failure (i.e. anemia, neutropenia, thrombocytopenia) and (ii) infiltration of organs (e.g. liver, spleen, lymph nodes, meninges, brain, skin or testes). Classification of leukemia: 1- Acute Leukemia: • Acute lymphoblastic leukemia: L1 – L3. • Acute myeloid leukemia: M0 – M7. 2- Chronic Leukemia: • Chronic lymphocytic leukemia. • Chronic myeloid leukemia. Dr. Rania Alhady
Acute leukemia Acute Leukemia: Definition: • Clonal malignant disorders characterized by: • Uncontrolled proliferation of abnormal blast cells in bone marrow, and • Impaired production of normal blood cells. • Blast cells infiltrate peripheral blood and bone marrow. • Blast cells in bone marrow must be > 30% to diagnose acute leukemia. Etiology: 1- Congenitaldisorder: • Down syndrome. • Immunodeficiency syndrome. 2- Ionizing radiation: X-ray, radiotherapy. 3- Chemicals: (alkylating agent, Benzene). 4- Viruses: Human T-lymphocyte leukemia virus (HTLV1), Herpes virus, EBV. Dr. Rania Alhady
Acute leukemia Results: * Chromosomalabnormality: • Imbalancebetweenoncogene and anti-oncogene. * Blast cells: Uncontrolledproliferation of this clone results in: 1- Arrest of cellular differentiation. 2- Reduced apoptosis. 3- Inhibition of normal marrow elements. Classification: Acute leukemias are classified according to the type of blast cells into: • ALL: Childhood leukemia. • AML: Adulthood leukemia. • Acute leukemias are fatal if not treated. • However, acute leukemias are easier to treat than chronic leukemias. Dr. Rania Alhady
Acute Lymphoblastic Leukemia Acute Lymphoblastic Leukemia (ALL): It is the result of clonal proliferation of lymphoid progenitor cells originating in the marrow. Incidence: Under 10 – 15 years (Childhood onset) • Can be either B-cell ALL or T-cell ALL. • B-cell ALL or T-cell ALL can be further classified into subtypesaccording to the moderate splenomegaly, hepatomegaly and meningeal syndrome. Classification of acute lymphoblastic leukemia (ALL) according to the French-American-British (FAB) groups Dr. Rania Alhady
Acute Lymphoblastic Leukemia Clinical features: 1- Bone marrow failure: • RBCs → Anemia: pallor, lethargy, malaise and dyspnea. • Leukocytes → neutropenia: fever, malaise, features of mouth, skin, respiratory infections. • Platelets → throbombocytopenia: spontaneous bruises, pupura, bleeding gums. 2- Tissue infiltration: • L.N. enlargement. • Hepatomegaly. More common with ALL than AML. • Splenomegaly. 3- Organ infiltration: A- Bony infiltration. B- Testicular infiltration. C- C.N.S. infiltration. 4- Fever. Dr. Rania Alhady
Acute Lymphoblastic Leukemia Investigations: 1- CBC: • 60% of patients have an elevated ↑↑ WBCs. • RBCs: ↓ Hb • Platelets: ↓ • Neutrpenia • 90% have lymphoblastsin the peripheral blood film. 2- Bone marrow: • BM Aspirate: • Hypercellular BM • All normal marrow elements are depressed and replaced by abnormal blasts. • 30% or more of all nucleated cells are blast B. BM Biopsy: Indicated in: • If aspirate is: a- Difficult. b- Hypercellular • Follow up. Dr. Rania Alhady
Acute Lymphoblastic Leukemia FAB Classification: Dr. Rania Alhad y
Acute Lymphoblastic Leukemia (a) L1 subtype-blasts show scanty cytoplasm without granules. (b) L2 subtype-blasts are larger and heterogeneous with more abundant cytoplasm. (c) L3 subtype-blasts are deeply basophilic with cytoplasmic vacuolation. Dr. Rania Alhady Morphological classification of ALL L1 L2 L3
Acute Lymphoblastic Leukemia 3- Immunophenotyping: Antigen present in the cell membrane A- Myeloid markers:-veCD13, CD33 B- Pan B markers:+veCD19, CD20, CD22 C- Pan T markers: +veCD2, CD5, CD7 4- Cytogenetics: • Philadelphia chromosome translocation t(9; 22): may occur and results in poor prognosis. 5- Cytochemistry: Chemical activity of the cell. • Myeloperoxidas, Sudan Black B, Non-specific estrase: -ve • Acid phosphatase: +vein T-ALL • PAS (periodic acid shiff): +ve Dr. Rania Alhady
Acute Lymphoblastic Leukemia 6- Radiology: • CXR: mediastinal mass (T-cell ALL) • Osteopenia or lytic lesion 50% of patients with ALL.(itractable pain). Prognosis of ALL: Bad prognosis in: • WBCs: ↑ > 20.000 • Sex: boys due to testicular involvement. • Serum Ig ↓ (also ↑ incidence of T-ALL) • L2 & L3morphology. • Organomegaly • Cytogenetic abnormalities • T-ALL Dr. Rania Alhady
Acute Myeloid Leukemia Acute Myeloid Leukemia (AML): Definition: • Clonal proliferation of myeloid precursor cells with reduced capacity to differentiate into more mature cellular elements. • Results in accumulation of leukemic forms in bone marrow, peripheral blood, and other tissues. • Leads to reduction in RBCs, platelets, PMNs. • It occurs in several morphologic variants; each one has a characteristic clinical & lab. features (M0 – M7) Dr. Rania Alhady
Acute Myeloid Leukemia Incidence: AML is the most common leukemia in neonates. • 80% of AML is in adults. • 20% of AML is in children. Diagnosis: • Clinical Picture: • Anemia weakness and easy fatigue • Neutropenia infections • Thrombocytopenia gingival bleeding, ecchymoses, epistaxis, menorrhagia • Anorexia, weight loss, fever. • Organomegaly: • HSM in 1/3 of patients. • Lymphadenopathy is uncommon except in monocytic variants. Dr. Rania Alhady
Acute Myeloid Leukemia B. Laboratory diagnosis: Bone Marrow Exam: Aspiration and biopsy * Morphologic classification using cytochemistry and immunophenotyping Cytochemistry: • Peroxidase: +ve • Sudan black: +ve • Specific esterase: +ve Immunophenotyping: Pan myeloid markers: +ve CD13, CD33 * Cytogenetic analysis * Evaluation for presence of significant fibrosis, presence of granulomata Dr. Rania Alhady
Acute Myeloid Leukemia Diagnosis requires all of the following diagnostic components: • Documentation of bone marrow infiltration • Myeloid origin of the leukemic cells • FAB/WHO classification of the leukemia FAB Classifications M0: minimally differentiated M1: without maturation M2: with maturation. M3: promyelocytic. M4: myelomonocytic. M5: monoblastic M6: erythroleukemia M7: megakaryoblastic. Dr. Rania Alhady
Acute Myeloid Leukemia Dr. Rania Alhady
Acute Myeloid leukemia Dr. Rania Alhady