Download
1 / 61
620 likes | 812 Views
Serial imaging studies Recommend surgical excision if chest pain develops Surgical excision now EBUS-TBNA drainage Conventional TBNA drainage.

E N D
Serial imaging studies • Recommend surgical excision if chest pain develops • Surgical excision now • EBUS-TBNA drainage • Conventional TBNA drainage A 23 yo female comes to your clinic for your opinion for a bronchogenic cyst. The CT imaging report states: “6 cm posterior mediastinal lesion which given its location most likely represents a bronchopulmonary foregut duplication cyst, specifically a bronchogenic cyst.” On pulmonary evaluation she describes using her friend’s albuterol HFA inhaler a couple of times per month for some “squeaky breathing” and dyspnea. She denies any chest pain, hemoptysis, or inspiratory stridor. Q: What is your recommendation for management of this bronchogenic cyst? Question by Dr. Alejandro Aragaki-Nakahodo, MD
Serial imaging studies • Recommend surgical excision if chest pain develops • Surgical excision now • EBUS-TBNA drainage • Conventional TBNA drainage A 23 yo female comes to your clinic for your opinion for a bronchogenic cyst. The CT imaging report states: “6 cm posterior mediastinal lesion which given its location most likely represents a bronchopulmonary foregut duplication cyst, specifically a bronchogenic cyst.” On pulmonary evaluation she describes using her friend’s albuterol HFA inhaler a couple of times per month for some “squeaky breathing” and dyspnea. She denies any chest pain, hemoptysis, or inspiratory stridor. Q: What is your recommendation for management of this bronchogenic cyst? Question by Dr. Alejandro Aragaki-Nakahodo, MD
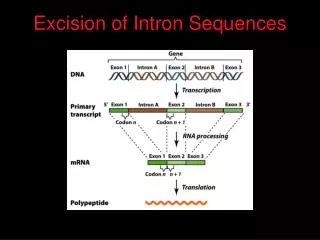
Management of bronchogenic cysts • According to Patel et al, complete surgical resection is the treatment of choice for both symptomatic and asymptomatic bronchogenic cysts out of concerns of late complications, particularly malignant transformation. • Eventually, all asymptomatic bronchogenic cysts will be symptomatic. • Patel et al noted a trend toward increased postoperative complications in patients who were symptomatic at the time of surgery. -This pt arguably already has symptoms Patel SR, Meeker DP, Biscotti CV et al. Presentation and Management of Bronchogenic Cysts in the Adult. Chest 1994;106:79-85 St. Georges R, Deslauriers J, Duranceau A et al. Clinical Spectrum of Bronchogenic Cysts of the Mediastinum and Lung in the Adult. Ann ThoracSurg1991;52:6-13 Cioffi U, Bonavina L, De Simoni M et al. Presentation and Surgical Management of Bronchogenic and Esophageal Duplication Cysts in Adults. Chest 1998; 113 (6): 1492-6 Question by Dr. Alejandro Aragaki-Nakahodo, MD
What constitutes a significant threshold score on the ACT questionnaire to prompt a patient to discuss possible poor control of asthma with their doctor? A) 22 or greater B) 19 or greater C) 15 or greater D) 22 or less • 19 or less • 15 or less Question by Dr. Peter Lenz, MD
What constitutes a significant threshold score on the ACT questionnaire to prompt a patient to discuss possible poor control of asthma with their doctor? A) 22 or greater B) 19 or greater C) 15 or greater D) 22 or less • 19 or less • 15 or less Question by Dr. Peter Lenz, MD
Which of the P-V graphs shown below best represents trapped lung? A) Graph with black circles B) Graph with white circles C) Graph with black triangles D) Trapped lung is not represented on the figure below Question by Dr. Peter Lenz, MD
Which of the P-V graphs shown below best represents trapped lung? A) Graph with black circles B) Graph with white circles C) Graph with black triangles D) Trapped lung is not represented on the figure below Question by Dr. Peter Lenz, MD
What is the elastance of the curve represented by black triangles? A) 4 L / cm H2O B) 4 cm H2O/L C)19 cm H2O/L D) 49 cm H2O/L E) 216 cm H2O/L Question by Dr. Peter Lenz, MD
What is the elastance of the curve represented by black triangles? A) 4 L / cm H2O B) 4 cm H2O/L C)19 cm H2O/L D) 49 cm H2O/L E) 216 cm H2O/L Question by Dr. Peter Lenz, MD
Elastance = Inverse of Compliance C= ∆V / ∆P E= ∆P / ∆V For this patient, E= 58 cm H2O/ 0.268 L = 216 H2O/L Question by Dr. Peter Lenz, MD
“The Unexpandable Lung” at: Chestnet.org http://www.chestnet.org/accp/pccsu/unexpandable-lung?page=0,3 Question by Dr. Peter Lenz, MD
Total time physician spends with patient/family. Total time occupied by family talking. Total time occupied by physician talking. Total time occupied by palliative care team member talking. Total time spent discussing hospice options. None of the above have been shown to improve family satisfaction. Which one of the following options below has been shown to have the most positive effect on family satisfaction scores regarding ICU end-of-life communication sessions with their critical care physicians? Question by Dr. Peter Lenz, MD
Total time physician spends with patient/family. Total time occupied by family talking. Total time occupied by physician talking. Total time occupied by palliative care team member talking. Total time spent discussing hospice options. None of the above have been shown to improve family satisfaction. Which one of the following options below has been shown to have the most positive effect on family satisfaction scores regarding ICU end-of-life communication sessions with their critical care physicians? Question by Dr. Peter Lenz, MD
Crit Care Med. 2004;32(7):1484 Question by Dr. Peter Lenz, MD
A 25-year-old male comes to your clinic to discuss smoking cessation. Spirometry was normal on prevous visit and his MCCT showed a PD20 of 18.2. Upon interviewing him he reveals that he smokes around five tobacco cigarettes per day and 2-3 hand-rolled marijuana cigarettes per month. He realizes that smoking tobacco can lead to COPD as his aunt has "horrible lungs and emphysema." He understands smoking can lead to COPD and has decided to quit smoking tobacco cigarettes, but also wants to know the risk of marijuana smoking. Which of the following statements below is most appropriate? A. This patient's marijuana habit does not have a significant risk of leading to airways obstruction. B. His marijuana habit is just as likely to lead to COPD as was his previous tobacco smoking. C. As long as he smokes from rolled marijuana cigarettes his marijuana smoking does not have deleterious effects to the lung. D. You applaud his efforts on quitting tobacco smoking and let him know that he can smoke up to 5-6 marijuana cigarettes a day without significant risk of lung injury. Question by Dr. Peter Lenz, MD
A 25-year-old male comes to your clinic to discuss smoking cessation. Spirometry was normal on prevous visit and his MCCT showed a PD20 of 18.2. Upon interviewing him he reveals that he smokes around five tobacco cigarettes per day and 2-3 hand-rolled marijuana cigarettes per month. He realizes that smoking tobacco can lead to COPD as his aunt has "horrible lungs and emphysema." He understands smoking can lead to COPD and has decided to quit smoking tobacco cigarettes, but also wants to know the risk of marijuana smoking. Which of the following statements below is most appropriate? A. This patient's marijuana habit does not have a significant risk of leading to airways obstruction. B. His marijuana habit is just as likely to lead to COPD as was his previous tobacco smoking. C. As long as he smokes from rolled marijuana cigarettes his marijuana smoking does not have deleterious effects to the lung. D. You applaud his efforts on quitting tobacco smoking and let him know that he can smoke up to 5-6 marijuana cigarettes a day without significant risk of lung injury. Question by Dr. Peter Lenz, MD
What constitutes a significant threshold score on the CAT questionnaire to determine possible poor control of COPD? A) 80 or greater B) 40 or greater C) 10 or greater D) 80 or less • 40 or less • 10 or less Question by Dr. Peter Lenz, MD
What constitutes a significant threshold score on the CAT questionnaire to determine possible poor control of COPD? A) 80 or greater B) 40 or greater C) 10 or greater D) 80 or less • 40 or less • 10 or less Question by Dr. Peter Lenz, MD
From: http://www.catestonline.org/ Question by Dr. Peter Lenz, MD
New GOLD Criteria http://medobserver.com/archivearticle.php?ArticleID=622 Question by Dr. Peter Lenz, MD
CAT questionnaire question • <10 = doing pretty well • 10-20 not so hot – needs optimisation • 20-30 really needs intervention • 30-40 BADLY needs intervention/specialist Question by Dr. Peter Lenz, MD
What is the most appropriate test to initiate an investigation for ABPA? • Serum total IgE • Specific IgE to Aspergillus species • Skin prick testing • Chest CT, non-contrast • Chest CT, contrasted Question by Dr. Peter Lenz, MD
What is the most appropriate test to initiate an investigation for ABPA? • Serum total IgE • Specific IgE to Aspergillus species • Skin prick testing • Chest CT, non-contrast • Chest CT, contrasted Question by Dr. Peter Lenz, MD
Stepwise Approach= A-SP-E-R-G illus Asthma Skin-Prick Test IgE level total Radiograph Globulins “Minimal Essential Criteria for ABPA” (-) (great NPV= if neg you are done; not ABPA) (+) (>417 IU/mL) & IgE & IgA specific to Aspergillus fumigatus >2X asthma controls distinguishes ABPA vs asthma w/ sensitiz Note: #5 Left = ABPA-CB vs 1-4 met = ABPA-SP Apter AJ et al. J All Clin Imm 1989; 84: 367-72. Question by Dr. Peter Lenz, MD
A 54-year-old male smoker comes to your clinic to discuss smoking cessation. He has tried with a few attempts before to quit but has never gotten past three months before taking up the habit again. He is disappointed and somewhat dismayed that he has not been able to quit smoking. A friend also told him that it will not matter if he quits smoking because his "lungs are already as bad as they're going to get". He is interested in smoking cessation but wants to know if he can get any changes in his lungs and when to expect these changes. You continue to talk with him about the natural decline in lung function and the acceleration of this lung function decline in smokers. Which of the following statements most accurately describes what this smoker can expect if he quits smoking? A. He is already over the age of 35, his lung function continues to decline, and smoking cessation will not have a significant impact on changing his lung function decline. B. The fact that he has tried to quit three times is very worrisome and will most likely preclude him from quitting C. Many smokers take multiple quit attempts and he should not be discouraged. His FEV1 could go back to normal after five years of smoking cessation. D. Many smokers take multiple attempts to quit and he should not be discouraged. His rate of lung function decline will be the same as a nonsmoker after five years of quitting. E. His risk for lung cancer will be the same as that of a nonsmoker after five years of quitting smoking. Question by Dr. Peter Lenz, MD
A 54-year-old male smoker comes to your clinic to discuss smoking cessation. He has tried with a few attempts before to quit but has never gotten past three months before taking up the habit again. He is disappointed and somewhat dismayed that he has not been able to quit smoking. A friend also told him that it will not matter if he quits smoking because his "lungs are already as bad as they're going to get". He is interested in smoking cessation but wants to know if he can get any changes in his lungs and when to expect these changes. You continue to talk with him about the natural decline in lung function and the acceleration of this lung function decline in smokers. Which of the following statements most accurately describes what this smoker can expect if he quits smoking? A. He is already over the age of 35, his lung function continues to decline, and smoking cessation will not have a significant impact on changing his lung function decline. B. The fact that he has tried to quit three times is very worrisome and will most likely preclude him from quitting C. Many smokers take multiple quit attempts and he should not be discouraged. His FEV1 could go back to normal after five years of smoking cessation. D. Many smokers take multiple attempts to quit and he should not be discouraged. His rate of lung function decline will be the same as a nonsmoker after five years of quitting. E. His risk for lung cancer will be the same as that of a nonsmoker after five years of quitting smoking. Question by Dr. Peter Lenz, MD
The 54-year-old male smoker comes back to your clinic to discuss smoking cessation some more. He is concerned becuase he doesn’t know if he “has it in himself to quit” and he goes on further to state that “quitting at my age ain’t going to help me anyway.” Which of the following statements most accurately describes what this smoker can expect in regards to his risk reduction and expectations for smoking cessation? A. His risk for lung cancer will be the same as that of a nonsmoker after five years of quitting smoking B. Quitting smoking near middle age still has significant health benefits and he could begin to reap lung cancer risk reduction after 5 years of smoking cessation. C. His FEV1 can get back to normal after 5 years of smoking cessation, and FVC after 3 years. D. At age 74 he will have the same lung cancer risk as a nonsmoker E. The weight gain he can expect from smoking cessation will lead to an increased risk of coronary artery disease, thus proving his thoughts correct. Question by Dr. Peter Lenz, MD
The 54-year-old male smoker comes back to your clinic to discuss smoking cessation some more. He is concerned becuase he doesn’t know if he “has it in himself to quit” and he goes on further to state that “quitting at my age ain’t going to help me anyway.” Which of the following statements most accurately describes what this smoker can expect in regards to his risk reduction and expectations for smoking cessation? A. His risk for lung cancer will be the same as that of a nonsmoker after five years of quitting smoking B. Quitting smoking near middle age still has significant health benefits and he could begin to reap lung cancer risk reduction after 5 years of smoking cessation. C. His FEV1 can get back to normal after 5 years of smoking cessation, and FVC after 3 years. D. At age 74 he will have the same lung cancer risk as a nonsmoker E. The weight gain he can expect from smoking cessation will lead to an increased risk of coronary artery disease, thus proving his thoughts correct. Question by Dr. Peter Lenz, MD
The Fletcher-Peto Graph Fletcher and Peto’s graph clearly shows the importance of smoking cessation, even in late stage COPD. Taken from: http://www.spirometrie.info/goldcopd.html Question by Dr. Peter Lenz, MD
From Up To Date • Smoking cessation reduces the accelerated decline of lung function and risk of incident COPD associated with smoking • In addition, the majority of smokers with cough and sputum production with early COPD have an improvement in symptoms in the first 12 months after cessation Question by Dr. Peter Lenz, MD
Smoking cessation — Smoking cessation clearly decreases the risk of lung cancer [15,22,23]. Large cohort and case-control studies have attempted to quantify the magnitude of the reduction in risk of lung cancer following cessation of smoking [22]: • Estimates of the extent of risk reduction over time vary from 20 to 90 percent, depending upon the duration of abstinence, with a progressive decline in risk associated with an increasing duration of abstinence. • An exception to the above pattern is an apparent increase in lung cancer risk within the first few years of abstinence, thought possibly to reflect the presence of symptoms of illness that led to smoking cessation prior to the diagnosis. • The reduction in risk becomes evident within five years of becoming abstinent [24]. **BUT NOT EQUAL TO THAT OF A NON-SMOKER in 5 YRS • Case-control studies show that former smokers who had been abstinent for more than 15 years had an 80 to 90 percent reduction in risk of lung cancer compared to current smokers [22,25]. However, lung cancer risk remains higher than that in the never smoker, even after prolonged periods of complete abstinence from smoking. It has been estimated that former smokers continue to have a 10 to 80 percent greater risk than never smokers [24]. (See "Patterns of tobacco use".) Question by Dr. Peter Lenz, MD
BMJ 2000 Question by Dr. Peter Lenz, MD
Tobacco Cessation One-Liners • There are huge benefits to quitting smoking – even well into middle age • Can reduce almost all of their lung CA risk if they stop by age 30 • Rate of FEV1 decline to that of a nonsmoker in 5 yrs (Peto-Fletcher graph) Question by Dr. Peter Lenz, MD
A 44-year-old Caucasian male presents to your clinic with productive cough, fatigue, and low grade subjective fevers as well as exertional dyspnea that is worsened to the point where he is now short of breath at rest. Nothing like this has ever happened to the patient before. Symptoms have occurred over the past six months and preliminary evaluation revealed the imaging showed in A and B on the right. Subsequent to this the patient produced five sputum cultures, all on separate days and three of them were positive for growth with mycobacterium avium-intracellulare complex. The patient’s pulmonary function tests have revealed mild obstruction and despite quitting smoking three months ago the patient has continued to have deteriorating symptoms. Which of the following management options (listed on next page) would be most preferred? Question by Dr. Lisa Haglund, MD
Which of the following antimicorbial management options would be most preferred? a. Rifampin, azithromycin and Streptomycin, given daily. b. Rifampin, Ethambutol and isoniazid, given once weekly. c. Rifampin, Ethambutol and isoniazid, given twice weekly. d. Rifampin, Ethambutol, clarithromycin given thrice weekly. e. Rifampin, Ethambutol and clarithromycin, given daily. f. Therapy not indicated at this time. Question by Dr. Lisa Haglund, MD
Which of the following antimicorbial management options would be most preferred? a. Rifampin, azithromycin and Streptomycin, given daily. b. Rifampin, Ethambutol and isoniazid, given once weekly. c. Rifampin, Ethambutol and isoniazid, given twice weekly. d. Rifampin, Ethambutol, clarithromycin given thrice weekly. e. Rifampin, Ethambutol and clarithromycin, given daily. f. Therapy not indicated at this time. Question by Dr. Lisa Haglund, MD
Answer E • Explanation; pt needs daily therapy because it is fibrocavitary MAI. the backbone of therapy for MAI treatment includes a macrolide, which in this particular question the clarithromycin containing regimen was most appropriate. • Daily therapy is more optimal vs thrice weekly for this patient because this patient has fibrocavitary disease. http://www.itd.unair.ac.id/files/ebook/Tuberculosis,%205th%20Edition/Tuberculosis,%205th%20Edition/HTML/34.htm Question by Dr. Lisa Haglund, MD
Fig. 34.4. Chest radiograph (A) and CT scan (B) from a patient with “classic” type pulmonary MAC. The chest radiograph demonstrates fibronodular upper lobe opacities, and cavitation is evident on the CT scan. http://www.itd.unair.ac.id/files/ebook/Tuberculosis,%205th%20Edition/Tuberculosis,%205th%20Edition/HTML/34.htm
A 49 y/o white female presents to the clinic after referral from her PCP for abnormal CT of the chest that was obtained to follow up for resolution of pneumonia. She was hospitalized 13 weeks ago for pneumonia (quant sputum cultures positive for strep pneumoniae > 100,000), and showed extensive bilateral lower lobe bronchiectasis. She c/o cough productive of yellow/green sputum for 10 plus years and has occasional blood tinged sputum and currently feels that her symptoms are at her baseline. She is married with 3 biological children and works as a cashier. PMH: Diabetes, Autoimmune thyroiditis and has had 2 hospitalizations for pneumonia other then the most recent. ROS Positive for Chronic cough with sputum production, sinus congestion and occasional diarrhea Exam T-98.3 HR-86 rr-12 bp-111/64 thin white female breathing comfortable on room air, b/l clubbing of the nails, 2 areas of skin 1 on the left arm and 1 on the back that are hypopigmented, no wheezing, basilar crackles Labs: CBC normal except for platelet count of 72, normal differential total IGE normal HIV and TB skin negative sweat chloride normal Spirometry shows no obstructive defect Bronchoscopy with BAL 6 weeks ago showed strep pneumoniae >100,000 AFB negative and cultures show no AFB organisms Which one of the following tests is the next appropriate step in establishing a diagnosis for this patient? Question by Dr. W. Ben Cundiff, MD
Which one of the following tests is the next appropriate step in establishing a diagnosis for this patient? a. HRCT of the chest b. Skin test for aspergillus c. Quantitative immunoglobulins d. IGG subclass levels e. Nasal brush biopsy Question by Dr. W. Ben Cundiff, MD
Which one of the following tests is the next appropriate step in establishing a diagnosis for this patient? a. HRCT of the chest b. Skin test for aspergillus c. Quantitative immunoglobulins d. IGG subclass levels e. Nasal brush biopsy Question by Dr. W. Ben Cundiff, MD
Answer: C. Quant Ig’s • The patient most likely has common variable immunodeficiency (CVID). Pt's usally have other autoimmune related diseases and are at risk for lymphomas. The correct answer is C. • C over B because you start with the Quantitative before ordering the subclass levels. Pt's with CVID must have the 4 following: • 1) Reduced total serum concentrations of IgG • 2) Low IgA or IgM or both • 3) Poor or no response to immunization • 4) No other immunodeficiency state. • The other answers are tests looking for other causes of bronchiectasis and reoccuring pneumonia which based on the history and the provided test results can be ruled out. J Allergy Clin Immunol. 2009; 124:1161. ClinImmunol. 1999; 93:190 CurrOpinPediatr. 1993;5(6):696. Question by Dr. W. Ben Cundiff, MD
Who is the most appropriate to receive succinylcholine for rapid sequence intubation? A.) 62 yo male with DKA, hypercapnic respiratory failure with potassium 5.6 B.) 35 yo female with trauma one month ago who developed pneumonia at LTAC C.) 45 yo male with traumatic paraplegia 9 months ago who has aspiration pneumonia after overdose D.) 75 yo male with who suffered 60% burn 9 months ago who developed hypoxemic respiratory failure from pulmonary emboli Question by Dr. Kyle Darnell, MD
Who is the most appropriate to receive succinylcholine for rapid sequence intubation? A.) 62 yo male with DKA, hypercapnic respiratory failure with potassium 5.6 B.) 35 yo female with trauma one month ago who developed pneumonia at LTAC C.) 45 yo male with traumatic paraplegia 9 months ago who has aspiration pneumonia after overdose D.) 75 yo male with who suffered 60% burn 9 months ago who developed hypoxemic respiratory failure from pulmonary emboli Question by Dr. Kyle Darnell, MD