Download
1 / 57
990 likes | 5.02k Views
A case presentation on Acute Appendicitis in the young. Aldwin Ong MD070061 15 February 2011. General objectives. To present a case of a young patient with Acute Appendicitis. Specific Objectives. To discuss Acute Appendicitis in the young , in particular:

E N D
A case presentation onAcute Appendicitisin the young Aldwin Ong MD070061 15 February 2011
General objectives • To present a case of a young patient with Acute Appendicitis
Specific Objectives • To discussAcute Appendicitis in the young, in particular: • Pathophysiology of appendicitis • Signs and symptoms of AP in the young • Diagnosis of AP • Management principles of AP
General data • J.T.G. • 18 y/o • Male • Pasig City, Philippines • Primary Informant: Patient (Reliability: 75%)
Chief complaint • “Sobrangsakitnangtiyanko”
History of present illness Late evening 3 days PTA Patient had sudden onset intermittent low to mid back pain, PS 4/10, associated with new onset fever, Tmax 39.8. No dysuria, no vomiting no nausea. Paracetamol taken with temporary relief. No consults done.
History of present illness 2 days PTA Pain became more pronounced in the epigastric region, PS 6-7/10, still intermittent; back pain now relieved. With 3 episodes of loose watery stool, loss of appetite, still associated with high-grade fever. No vomiting, no dysuria. Paracetamol continued. No consults done.
History of present illness 1 day prior to consult Epigastric pain persisted, now also with RLQ pain, persistent, PS 8-9/10, associated with fever, anorexia, nausea. No more loose stool. Consult done at RMC. CBC and UA done. Impression was Acute Appendicitis, however, no vacant beds Admission
Review of systems General:no weight loss, no weakness, no fatigue MS & Skin: no other lumps/masses, no rashes, no sores, no itching, no arthralgia, no color changes HEENT: no headache, no dizziness, no enlarged lymph nodes, no cough, no colds
Review of systems Cardiovascular: no palpitations, no chest pain, no syncope Respiratory: no dyspnea, no hemoptysis, no shortness of breath, no cough, no wheezing Gastrointestinal: no vomiting, no jaundice
Review of systems Genitourinary:no edema, no dysuria, no frequency, no urgency Endocrine: no diaphoresis, no cold intolerance, no heat intolerance Nervous: no seizure, no tremor
Past medical history • Born with cleft lip • Repaired during infancy • Asthma, controlled • No medications being taken • No DM II • No known allergies • Immunization up-to-date • No other hospitalizations; no other surgeries
Family history • Asthma, DM, Hypertension • No known congenital diseases in the family
Personal & Social History • Denies smoking • Occasional alcoholic beverage drinker • Denies illicit drug use
Personal & Social History • Eldest of 3 children • Good relationship with parents and siblings • Stopped schooling at 2nd yr HS due to computer gaming • Since then has tried to work as a computer shop attendant • Attempted to go back to school, but dropped out soon after due to laziness • Currently not going to school or work • Likes to play basketball for his pastime
Physical examination General Survey: Awake, alert, not in apparent cardiorespiratory distress. Vital Signs: BP 90/60 HR 98 RR 20 T 39.2C
Physical examination • Skin: • Fair and even color, no rashes noted, good turgor • HEENT: • Pink palpebral conjunctivae, anictericsclerae. • No TPC, No CLAD. Flat neck veins.
Physical examination • Chest/Lungs: • symmetrical chest expansion, no retractions, resonant in all LF, clear breath sounds, no rales, no rhonchi, no wheezes • Heart: • adynamicprecordium, no heaves, no lifts, no thrills, PMI at 5th ICS LMCL, normal rate, regular rhythm, no murmur
Physical examination • Abdomen: • flat, hyperactive bowel sound, guarding, (+) direct and rebound tenderness at RLQ > epigastric area, (–) Rovsings Sign, (–) CVA tenderness, no hepatosplenomegaly, no palpable masses • Extremities: • No gross deformities, full and equal pulses, no edema • Rectum: • Not indicated • Genitalia: • Not indicated
Physical examination • Cerebrum: • GCS 15 • Conversant. Intact Sensorium. • Rest of neurologic exam unremarkable.
Salient Features • 18 y/o Male • 3 day history of migrating, progressive abdominal pain, noted initially at the lower back, then epigastric area, and eventually localizing at the RLQ, associated with high-grade fever, anorexia, loose bowel movement, and nausea. • With physical findings of abdominal guarding, hyperactive bowel sounds, direct and rebound tenderness at RLQ.
Initial Impression t/c Acute Appendicitis r/o Urinary Tract Infection r/o Acute Gastroenteritis r/o Dengue Fever
Diagnostics Done URINALYSIS RBC 4/hpf [0-2] WBC 2/hpf [0-2] EC 7/hpf [0-2] Casts 0/hpf Bact 1/hpf [0-20] • CBC • Urinalysis • Fecalysis • Dengue NS1 FECALYSIS Color Green Consistency Loose Mucus Positive Blood (G/O) Negative No Ova or Parasite seen Negative for Amoeba CBC Hgb 160 g/L Hct 0.48 WBC 7.6 N 0.86 L 0.09 M 0.05 Plt 193 DENGUE NS1 Negative
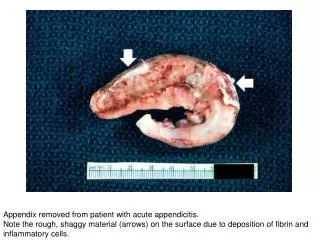
Final Diagnosis • Acute Appendicitis
Management • Open Appendectomy
Statistics • Acute appendicitis is the most common condition requiring emergency abdominal operation in childhood. • Perforation rates in children = 30-60% • Greatest risk of perforation is in children 1-4 year old (70-75%) • Lowest risk of perforation is in the adolescent age group • The adolescent age group has the highest age-specific incidence of appendicitis in childhood
Epidemiology • 6% of population, M>F • 80% between 5-35 years of age
Operative Definitions • Uncomplicated Appendicitis - includes the acutely inflamed, phlegmonous, suppurative, or mildly inflamed appendix with or without peritonitis • Complicated Appendicitis - includes gangrenous appendicitis, perforated appendicitis, localized purulent collection at operation, generalized peritonitis and periappendiceal abscess • Equivocal Appendicitis – a patient with right lower quadrant abdominal pain who presents with an atypical history and physical examination and the surgeon cannot decide whether to discharge or to operate on the patient
Pathogenesis • luminal obstruction bacterial overgrowth inflammation/swelling increased pressure localized ischemia gangrene/perforation localized abscess (walled off by omentum) or peritonitis • In young children, the omentum is poorly developed • Perforation is not usually confined • Bacterial invasion of mesenteric veins • Portal vein sepsis and subsequent liver abscess may form • Inflammatory process intestinal obstruction or paralytic ileus
Etiology • Children or young adult: hyperplasia of lymphoid follicles, initiated by infection • Adult: fibrosis/stricture, fecolith, obstructing neoplasm • Other causes: parasites, foreign body
Symptoms • Common symptoms of appendicitis • abdominal pain • anorexia • nausea • constipation • vomiting • Vomiting less common with uncomplicated appendicitis • Profuse vomiting may indicate generalized peritonitis associated with perforation
Symptoms • Appendicitis in children is more difficult to recognize clinically than in adults: • abdominal pain is often poorly localized • small children are rarely able to describe their symptoms clearly
Symptoms • Children with appendicitis may have atypical history • Based on (2007) diagnostic cohort study 755 children enrolled over 20 month period • common clinical features reported in only 50%-68% children • pain migration in 50% • anorexia in 60% • maximal pain in right lower quadrant in 68% • 45% had abrupt onset of pain • In (1997) series of 63 children < 3 years old with appendicitis, 57% initially misdiagnosed • 33% had diarrhea as presenting symptom • 84% had perforation and/or gangrene
Diagnostic Management • Diagnosis of appendicitis is still highly based on history, and physical examination • Imaging modalities may be helpful • Blood parameter including CBC and CRP may also help • Mild leukocytosis with left shift (may have normal WBC counts) • Higher leukocyte count with perforation
Laboratory Tests • CBC • Mild leukocytosis with left shift • (may have normal WBC counts) • Higher leukocyte count with perforation • Urinalysis • To rule out urinary tract infection
Clinical Decision Rule • Clinical decision rule: • absolute neutrophil count > 6,750/mcL, OR • combination of nausea PLUS maximal tenderness in right lower quadrant • This rule appears sufficientlysensitive for appendicitis that children without these features can be observed without CT imaging
Pediatric Appendicitis Score (PAS) • The PAS predicts appendicitis in • > 70% children if score ≥ 7 and • Rules out appendicitis in > 99% patients with score < 2
Alvarado/MANTRELS • 9-10: almost certain, little advantage for further work-up • 7-8: high likelihood • 5-6: compatible but not diagnostic • 0-4: Unlikely
Equivocal Appendicitis in Pediatric Age Group Imaging modalities that may be used: • Ultrasound (Sensitive but not specific) • to confirm acute appendicitis but not to definitively rule out acute appendicitis • CT Scan (Sensitive and specific) • if diagnosis uncertain after ultrasound, use abdominal and pelvic CT to confirm or rule out acute appendicitis For pediatric patients, UTZ is preferred because of its: • lack of radiation • cost-effectiveness • availability compared to CT scan
Therapeutic Management • Definitive management for Acute Appendicitis in the Pediatric age group is Appendectomy via (PCS, 2002): 1. Open Appendectomy 2. Laparoscopic Appendectomy
Prophylaxis • Antibiotic prophylaxis (Adults vs. Children) • Uncomplicated AP • Cefoxitin 2 grams IV single dose (Adults) • 40 mg/kg IV single dose (Children) • Ampicillin-sulbactam 1.5-3 grams IV single dose (Adults) • 75 mg/kg IV single dose (Children) • Amoxicillin-clavulanate 1.2 –2.4 grams IV single dose (Adults) • 45 mg/kg IV single dose (Children)
Prophylaxis • For therapy of complicated appendicitis in pediatric patients: • Ticarcillin-clavulanic acid 75 mg/kg IV every 6 hours • Alternative agents for pediatric patients include: • Imipenem-Cilastatin 15-25 mg/kg IV every 6 hours • For children with beta-lactam allergy • Gentamicin 5 mg/kg IV every 24 hours plus Clindamycin 7.5 –10 mg/kg IV every 6 hours