Download
1 / 41
470 likes | 970 Views
ACUTE APPENDICITIS. Roy Phitayakorn, M.D. Christopher Brandt, M.D. Case Western Reserve University School of Medicine. Ms. Z. Cope. You are called to see a patient in the Emergency Department, who is a 25 year-old female with a 1 day history of right-lower quadrant abdominal pain. History.

E N D
ACUTE APPENDICITIS Roy Phitayakorn, M.D. Christopher Brandt, M.D. Case Western Reserve University School of Medicine
Ms. Z. Cope • You are called to see a patient in the Emergency Department, whois a 25 year-old female with a 1 day history of right-lower quadrant abdominal pain.
History What other points of the history do you want to know?
History, Ms. Cope Consider the Following • Characterization of symptoms • Temporal sequence • Alleviating / Exacerbating factors: • Pertinent PMH, ROS, MEDS. • Relevant family hx. • Associated signs and symptoms
Pain started in the middle of the night and woke the patient from sleep. Felt nauseated and vomited after pain No significant MED.HX. or SURG HX. Negative Family HX Noted some indigestion yesterday Feels urge to have bowel movement, but has been constipated History, Patient ZC
Differential DiagnosisBased on History and Presentation • Systemic or infectious conditions • Influenza • Gastroenteritis • Hepatitis • Diaphragmatic pleurisy • Spinal disease • Typhoid • Tuberculosis • Acute porphyria • Diabetic ketoacidosis
Differential Diagnosis(cont.) • Intra-abdominal conditions • Acute Appendicitis • Acute Cholecystitis • Diverticulitis (Meckel’s) • Inflammatory Bowel Disease (Crohn’s) • Duodenal Ulcer • Intestinal Obstruction • Carcinoma of the Cecum • Nonspecific adenitis – Possible Yersinia infection
Differential Diagnosis(cont.) • Intra-pelvic conditions • Salpingitis • Pelvic Inflammatory Disease • Ectopic Pregnancy • Ruptured Corpus Luteum Cyst • Ruptured Follicular Cyst (Mittelschmerz) • Ruptured Ovarian Cyst • Ovarian Torsion • Pyelonephritis • Ureteral/Renal stone
Physical Examination What would you look for?
Physical Examination, Patient ZC • Vital Signs: 39o C, HR=75, RR=15, BP=125/75 • Appearance: Patient is lying quietly on bed in fetal position
Would you like to revise your Differential Diagnosis? • Acute appendicits • Diverticulitis (Meckel’s) • Inflammatory Bowel Disease (Crohn’s) • Ovarian pathology • Acute cholecystitis • Intestinal obstruction • Nonspecific adenitis – Possible Yersinia infection
Laboratory What would you obtain?
Lab Results, Ms. Cope CBC: 14,500 LFTs : WNL HCG : WNL Electrolytes : WNL Amylase : WNL U/A: WNL
Interventions at this point?Consider the following • Start IV with Ringers Lactate or similar isotonic crystalloid solution • Administer antibiotics • Admit to the hospital • Go Directly to the OR? • Other?
Studies What further studies would you want at this time?
Radiologic Studies to Consider • Flat/Upright Abdomen • CT Scan: Abd/Pelvis • CT Scan: Other ? • US Abdomen/Pelvis
Considering your Differential Diagnosis • What would you expect to see on a flat/upright abdominal series? • What specific abnormalities do you look for on US? What population? • Are there specific CT findings in any of your top 3 diagnoses?
Abdominal X-ray Findings • Non-specific gas pattern • No fecalith • No free air
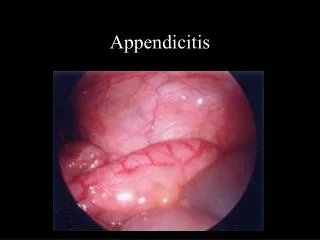
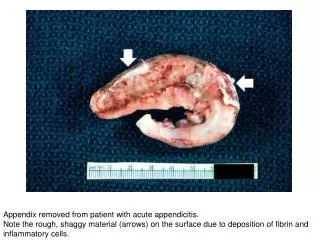
CT Scan – Results • Acute Appendicitis • Thickened dilated appendix • Peri-appendiceal fat stranding • Scant free fluid • Incidental small left ovarian cyst What is the differential diagnosis at this point?
What next? • Additional Imaging? • Observation? • OR? • Other?
What next? Discussion of suggested interventions
Management • Surgical Options • Pre-operative preparation
Discussion Pathophysiology of the disease process, visceral vs. parietal abdominal pain, laparoscopy vs. open, antibiotic management, appropriate utilization of resources, etc.
Discussion Additional teaching points
Alternative scenarios • Acute Appendicitis with perforation/ Abscess or tumor • IBD • Acute Diverticulitis • Ovarian Cyst / Torsion/ • Perforated Right colon tumor
Acknowledgment The preceding educational materials were made available through theASSOCIATION FOR SURGICAL EDUCATION In order to improve our educational materials wewelcome your comments/ suggestions at: feedbackPPTM@surgicaleducation.com