Download
1 / 15
150 likes | 163 Views
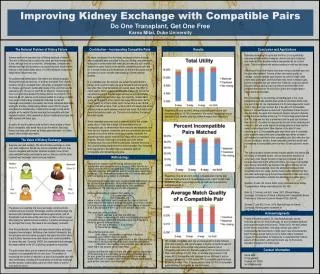
This article discusses the problem of end-stage renal disease and the shortage of kidney transplants. It explores the Top Trading Cycle with Chains method, patient rationality, multiple donors, and other considerations to improve the current system. The goal is to enhance patient welfare and alleviate the shortage of kidneys.

E N D
Kidney Exchange Enrichment Michael Levy David Flatow
The Problem • End Stage Renal Disease (ESRD) is a fatal disease unless treated with dialysis or kidney transplantation (preferred method) • 86,000 patients on the waiting list (Jan ‘09-Dec ’09) • Median wait time for transplant: 4 years • 4,600 patients died • 34,000 new patient registrations • 10,400 transplants of cadaver kidneys and 6,400 transplants of kidneys from living donors • Want to alleviate this shortage and improve patient welfare
The Problem (Cont’d) • Two genetic characteristics play key roles in the success of a kidney transplant • ABO blood-type • Type O can only receive type O • HLA (tissue) type • Mismatch decreases likelihood of successful graft (Opelz, 1997) • The presence of antibodies, called a positive crossmatch, effectively rules out transplantation
The Problem (Cont’d) • 1/3 of O donor kidneys go to non-O recipients • 1/3 of A recipients have O donors • ½ of B recipients have O donors
The Status Quo • Transplants from live donors generally have a higher chance of success than those from cadavers • A patient identifies a healthy, willing, feasible donor and the transplant it is carried out • Other types of exchanges • paired exchange • indirect exchange (list exchange) • market exchange • Can we do better?
Top Trading Cycle with Chains (TTCC) • Each remaining active patient points to his most preferred remaining unassigned kidney or to the wait-list option, whichever is more preferred • There is either a cycle, or a chain, or both. • Proceed to Step 3 if there are no cycles. Otherwise, remove all patients in a cycle together with their assignments. • Each remaining patient points to his top choice among remaining kidneys. Locate all cycles and remove them. Repeat until no cycle exists. • If there are no pairs left, we are done. Otherwise, remove only one of the chains with the chain selection rule. • After a w-chain is selected, new cycles may form. Repeat Steps 2 and 3 with the remaining active patients and unassigned kidneys until no patient is left.
Rationality • Patient Rationality (Roth et al, 2004) • depends HLA mismatches ( x) and donor age ( y) • “rational” u(x,y)=0.514x - y/10 • “cautious” IRs prefer other compatible Ds to his own only if they are more than an equivalent of one HLA mismatch better • Want to redefine “cautious” and explore benefits of incentive schemes of entering the market • Under Roth’s definition of “cautious”, an IR would join the kidney exchange even if they had a compatible D
Rationality (Cont’d) • Compatible pairs do not join the exchange (Gentry et al, 2007) • Participation of compatible pairs can double the match rate for incompatible pairs (Gentry et al, 2007) • Reflects preferences for a related donor, time constraints, and incomplete information • How can we get more compatible people to join?
Rationality (Cont’d) • “Opt Out” versus “Opt In” policy • Put everyone into the system • Can always leave at no cost • Updating preferences with possible matches • “Completing” their information • Updating preferences with possible matches • Less repugnant than “Opt Out”
Multiple Donors • Single Donors • Currently, each IR brings a single D to the exchange (Roth et al, 2004) • Optimizing which donor to bring • Want to allow each IR to bring multiple Ds • Only one donates (Roth et al, 2006) • Possibly multiple donate • Any D in a cycle or starts an altruistic chain donates • A certain number donates to an IR or the waitlist • All donate to an IR or the waitlist
Multiple Donors (Cont’d) • Roth et al, 2006 demonstrated efficiency gains when only one of your multiple Ds donates • Multiple people donating will create more efficiency • Is it too repugnant? • Are there incentives to bring less people? • Are there issues with reneging? • Conjecture: Having multiple Ds donate does not improve the kidney you receive compared to when only one of your multiple Ds donates
Multiple Donors (Cont’d) • Should people with more Ds donating get preferential treatment? • Do we lose stability? • Too repugnant? • Overcome the conjecture? • Multiple donating comes with several caveats • Concentrated risk • Logistical concerns • Stop people from incrementing their donor set?
Other Considerations • Stricter blood type matching • “Save” O kidneys for O patients, A for As, etc. • Donor Swapping • Your D donates to someone in exchange for their D to be paired with you • Altruistic Donors • Can we increase the amount of altruism? • Non-Simultaneous Extended Altruistic Donor Chains speak well about reneging