Download
1 / 43
770 likes | 2.42k Views
OBJECTIVES. Understand the role of arthropods in human diseaseRecognize arthropods implicated in important human diseasesDescribe important vector-borne diseases. WHAT ARE ARTHROPODS"?. Largest phylum of animals 80% of described animal species are arthropodsInclude insects, spiders, crustac

E N D
1. Arthropod Disease Surbhi Modi, MD, MPH
Preventive Medicine Resident
Emory University School of Medicine
September 20, 2007
2. OBJECTIVES Understand the role of arthropods in human disease
Recognize arthropods implicated in important human diseases
Describe important vector-borne diseases
I won�t be able to cover all of the arthropod-related diseases in the next hour, so I will just give a highlight of some of the most interesting and clinically relevanyI won�t be able to cover all of the arthropod-related diseases in the next hour, so I will just give a highlight of some of the most interesting and clinically relevany
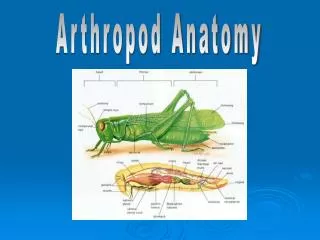
3. WHAT ARE �ARTHROPODS�? Largest phylum of animals � 80% of described animal species are arthropods
Include insects, spiders, crustaceans Arthropods represent the largest phylum of animals and include the insects, arachnids, crustaceans, and others. Arthropods are characterized by the possession of a segmented body with appendages on each segment. All arthropods are covered by a hard exoskeleton made of chitin, which provides physical protection and resistance to desiccation.
More than 80% of described living animal species are arthropods�and there are over a million modern species described. Arthropods are common throughout marine, freshwater, terrestrial, and even aerial environments.
Pic: http://en.wikipedia.org/wiki/InsectArthropods represent the largest phylum of animals and include the insects, arachnids, crustaceans, and others. Arthropods are characterized by the possession of a segmented body with appendages on each segment. All arthropods are covered by a hard exoskeleton made of chitin, which provides physical protection and resistance to desiccation.
More than 80% of described living animal species are arthropods�and there are over a million modern species described. Arthropods are common throughout marine, freshwater, terrestrial, and even aerial environments.
Pic: http://en.wikipedia.org/wiki/Insect
4. MEDICAL ENTOMOLOGY Direct parasitism or injury
Indirect injury as disease vectors Medical entomology is the study of arthropods � including insects, spiders, ticks, and mites -- and the diseases they transmit
There are two main mechanisms for human harm from arthropods that we will discuss today:
1. Direct parasitism, injury, irritation or annoyance by the arthropod itself
2. Indirect injury by the vectoring of disease agents. The two pictures on the left illustrate two examples of arthropods that act as disease vectors:
In the top picture, we see: Aedes aegypti, a parasite, and vector of dengue fever and yellow fever
In the bottom picture, we see: an electron micrograph photo of a flea, the disease vector in plague
Medical entomology is the study of arthropods � including insects, spiders, ticks, and mites -- and the diseases they transmit
There are two main mechanisms for human harm from arthropods that we will discuss today:
1. Direct parasitism, injury, irritation or annoyance by the arthropod itself
2. Indirect injury by the vectoring of disease agents. The two pictures on the left illustrate two examples of arthropods that act as disease vectors:
In the top picture, we see: Aedes aegypti, a parasite, and vector of dengue fever and yellow fever
In the bottom picture, we see: an electron micrograph photo of a flea, the disease vector in plague
5. DIRECT DISEASE AGENTS First, we�ll discuss the arthropod as a direct disease agent. Arthropods may affect human health directly by bites, stings, or infestation of tissues. I will focus on only a few interesting, clinically relevant examples.First, we�ll discuss the arthropod as a direct disease agent. Arthropods may affect human health directly by bites, stings, or infestation of tissues. I will focus on only a few interesting, clinically relevant examples.
6. SCABIES Caused by the mite Sarcoptes scabei
Mites burrow under the skin � takes <3 minutes
Linear burrows that contain mites & their eggs
Especially in the webbing between fingers and the folds of the wrists
Genital lesions common
Spread by skin-skin contact
Secondary infections
Norwegian scabies
Scabies is caused by the mite Sarcoptes scabiei,
The pregnant female mite tunnels into the skin and deposits eggs into linear burrows.
The larvae, which hatch in 3-10 days, move about on the skin, molt into a "nymphal" stage, and then mature into adult mites. The adult mites live 3-4 weeks in the host's skin.
The movements of the mites and the presence of the eggs produces a massive allergic response. In someone who has never been exposed to scabies, the allergic response may be delayed up to 4 weeks. However, the individual is still contagious in this first month.
A delayed hypersensitivity (allergic) response resulting in a papular eruption (red, elevated area on skin) often occurs.
While there may be hundreds of papules, fewer than 10 burrows are typically found. The burrow appears as a fine, wavy and slightly scaly line a few millimeters to one centimeter long. A tiny mite (0.3 to 0.4 mm) may sometimes be seen at the end of the burrow.
The most common areas for burrows are hands, wrists, elbows. The pathognomic genital lesions includes crusted, excoriated pruritic papules on the penis or buttocks
Scabies is transmitted easily by skin-to-skin contact with an infected person (household contacts, schoolmates, and children in daycare are especially susceptible).
Spread by clothing, bedding, or towels is a less significant risk, but this is also possible.
The rash may become secondarily infected; scratching the rash may break the skin and make secondary infection more likely.
In persons with severely reduced immunity, such as those with HIV infection, or people being treated with immunosuppressive drugs like steroids, a widespread rash with thick scaling � called Norwegian scabies -- may result. This variety of scabies often has no burrows.
Photo taken at 100x magnification through a microscope of a scabies mite (Sarcoptes scabiei). http://en.wikipedia.org/wiki/ScabiesScabies is caused by the mite Sarcoptes scabiei,
The pregnant female mite tunnels into the skin and deposits eggs into linear burrows.
The larvae, which hatch in 3-10 days, move about on the skin, molt into a "nymphal" stage, and then mature into adult mites. The adult mites live 3-4 weeks in the host's skin.
The movements of the mites and the presence of the eggs produces a massive allergic response. In someone who has never been exposed to scabies, the allergic response may be delayed up to 4 weeks. However, the individual is still contagious in this first month.
A delayed hypersensitivity (allergic) response resulting in a papular eruption (red, elevated area on skin) often occurs.
While there may be hundreds of papules, fewer than 10 burrows are typically found. The burrow appears as a fine, wavy and slightly scaly line a few millimeters to one centimeter long. A tiny mite (0.3 to 0.4 mm) may sometimes be seen at the end of the burrow.
The most common areas for burrows are hands, wrists, elbows. The pathognomic genital lesions includes crusted, excoriated pruritic papules on the penis or buttocks
Scabies is transmitted easily by skin-to-skin contact with an infected person (household contacts, schoolmates, and children in daycare are especially susceptible).
Spread by clothing, bedding, or towels is a less significant risk, but this is also possible.
The rash may become secondarily infected; scratching the rash may break the skin and make secondary infection more likely.
In persons with severely reduced immunity, such as those with HIV infection, or people being treated with immunosuppressive drugs like steroids, a widespread rash with thick scaling � called Norwegian scabies -- may result. This variety of scabies often has no burrows.
Photo taken at 100x magnification through a microscope of a scabies mite (Sarcoptes scabiei). http://en.wikipedia.org/wiki/Scabies
7. SCABIES Left: This is a picture of scabies after 6 days of untreated infestation. Many itchy red patches visible.
Right: A scabies burrow under magnification. The scaly patch at the left is due to scratching of the original papule. The mite traveled from there to the upper right, where it can be seen as a dark spot at the end of the burrow. Left: This is a picture of scabies after 6 days of untreated infestation. Many itchy red patches visible.
Right: A scabies burrow under magnification. The scaly patch at the left is due to scratching of the original papule. The mite traveled from there to the upper right, where it can be seen as a dark spot at the end of the burrow.
8. SCABIES Clinical diagnosis, but can confirm by microscopy
Treatment:
Ivermectin
Lindane, Permethrin, Crotamiton
Prevent Re-infection
Treat ALL family & close contacts
Clean environment
Warn patients that itching may continue for 2 � 4 weeks after treatment initiated The diagnosis of scabies is usually a clinical one
When a suspected burrow is found, diagnosis may be confirmed by microscopy of surface scrapings, which are placed on a slide in glycerol, mineral oil or immersion in oil and covered with a coverslip.
Treatment usually involves topical pesticides but oral ivermectin is a newer option
It is critical to Prevent Reinfection
- All family and close contacts should be treated at the same time, even if asymptomatic.
- Without a host, scabies mites can on average survive up to 4 days away from human skin.
- Therefore it is recommended, after treatment, to wash all material (such as clothes and bedding) that has been in contact with all infested
persons in the last five days � use the hottest water possible
- Vacuum floors, carpets, rugs, mattresses and furniture daily
- Disinfect floor and bathroom surfaces
It�s also important to warm patients that they should expect itching to continue for a few weeks as the eggs die � this does not mean that treatment is not effective
The diagnosis of scabies is usually a clinical one
When a suspected burrow is found, diagnosis may be confirmed by microscopy of surface scrapings, which are placed on a slide in glycerol, mineral oil or immersion in oil and covered with a coverslip.
Treatment usually involves topical pesticides but oral ivermectin is a newer option
It is critical to Prevent Reinfection
- All family and close contacts should be treated at the same time, even if asymptomatic.
- Without a host, scabies mites can on average survive up to 4 days away from human skin.
- Therefore it is recommended, after treatment, to wash all material (such as clothes and bedding) that has been in contact with all infested
persons in the last five days � use the hottest water possible
- Vacuum floors, carpets, rugs, mattresses and furniture daily
- Disinfect floor and bathroom surfaces
It�s also important to warm patients that they should expect itching to continue for a few weeks as the eggs die � this does not mean that treatment is not effective
9. BROWN RECLUSE SPIDER BITES Found in midwest & south-central US
�Reclusive� nature
Found inside shoes, clothing, attics, cardboard boxes, etc.
Be careful of misdiagnosis!
Next we�ll talk about the bite of two different spiders: the brown recluse spider & the black widow spider
The brown recluse spider is distinguished by violin-like markings -- (I don�t see it but maybe you do?)
The brown recluse spider is the most widespread of the North American recluse spiders and lives in the south central Midwest from Nebraska to Ohio and south through Texas to Georgia. It is rarely found west of the Rockies.
As their name implies, these spiders are �reclusive� in nature
They prefer to hide in dark, dry places & usually bite when someone unsuspectingly disturbs their hiding place while cleaning out an attic or putting their foot in a shoe
True brown recluse spider bites are rare though and many other conditions are often misdiagnosed as spider bites. Nationwide, some "brown recluse bites" were subsequently correctly diagnosed as Staphylococcus infection, Streptococcus ("flesh-eating bacteria") infection, Lyme disease, herpes simplex, diabetic ulcer, or bites from other arthropods.
As an aside, brown recluse spider bite is also in the differential diagnosis of cutaneous anthrax
http://en.wikipedia.org/wiki/Brown_recluse_spider
http://www.ipm.ucdavis.edu/PMG/PESTNOTES/pn7468.html
Next we�ll talk about the bite of two different spiders: the brown recluse spider & the black widow spider
The brown recluse spider is distinguished by violin-like markings -- (I don�t see it but maybe you do?)
The brown recluse spider is the most widespread of the North American recluse spiders and lives in the south central Midwest from Nebraska to Ohio and south through Texas to Georgia. It is rarely found west of the Rockies.
As their name implies, these spiders are �reclusive� in nature
They prefer to hide in dark, dry places & usually bite when someone unsuspectingly disturbs their hiding place while cleaning out an attic or putting their foot in a shoe
True brown recluse spider bites are rare though and many other conditions are often misdiagnosed as spider bites. Nationwide, some "brown recluse bites" were subsequently correctly diagnosed as Staphylococcus infection, Streptococcus ("flesh-eating bacteria") infection, Lyme disease, herpes simplex, diabetic ulcer, or bites from other arthropods.
As an aside, brown recluse spider bite is also in the differential diagnosis of cutaneous anthrax
http://en.wikipedia.org/wiki/Brown_recluse_spider
http://www.ipm.ucdavis.edu/PMG/PESTNOTES/pn7468.html
10. BROWN RECLUSE SPIDER BITES
Painless bite
Followed by erythema, swelling, tenderness The bite itself is usually painless. Symptoms tend to begin about 3 � 8 hours later and the site becomes red, swollen, tender. The initial cellulitis/rash/blister becomes a black scab and ulcerates
The bite itself is usually painless. Symptoms tend to begin about 3 � 8 hours later and the site becomes red, swollen, tender. The initial cellulitis/rash/blister becomes a black scab and ulcerates
11. BROWN RECLUSE SPIDER BITE Skin necrosis
Sphingomyelinase D
Rare systemic reactions
Routine treatment
Dapsone?
Antivenom not widely available
As you can see here, the cellulitis has progressed to necrosis.
Black recluse venom contains sphingomyelinase D � which is a dermonecrotic factor that activates platelet aggregation, thrombosis & massive neutrophil infiltration
Very rarely, victims have a systemic reaction � characterized by hematuria, anemia, fever, rash, nausea, vomiting, coma, and cyanosis
Treatment:
- Routine treatment should include elevation and immobilization of the affected limb, application of ice, local wound care, and tetanus prophylaxis. In almost all cases, bites are self-limited and typically heal without any medical intervention.
- Dapsone has been used with varying degrees of success. No randomized clinical trials & cannot use with G6PD deficiency
- Studies have shown surgical intervention is ineffective and may worsen outcome. Excision may delay wound healing, cause abscesses, and lead to disfiguring scarring.
- Antivenom is not widely available but does appear to be the most promising therapy. However, antivenoms are most effective if given early and because of the painless bite patients do not often present until 24 or more hours after the event, possibly limiting the effect of this intervention.As you can see here, the cellulitis has progressed to necrosis.
Black recluse venom contains sphingomyelinase D � which is a dermonecrotic factor that activates platelet aggregation, thrombosis & massive neutrophil infiltration
Very rarely, victims have a systemic reaction � characterized by hematuria, anemia, fever, rash, nausea, vomiting, coma, and cyanosis
Treatment:
- Routine treatment should include elevation and immobilization of the affected limb, application of ice, local wound care, and tetanus prophylaxis. In almost all cases, bites are self-limited and typically heal without any medical intervention.
- Dapsone has been used with varying degrees of success. No randomized clinical trials & cannot use with G6PD deficiency
- Studies have shown surgical intervention is ineffective and may worsen outcome. Excision may delay wound healing, cause abscesses, and lead to disfiguring scarring.
- Antivenom is not widely available but does appear to be the most promising therapy. However, antivenoms are most effective if given early and because of the painless bite patients do not often present until 24 or more hours after the event, possibly limiting the effect of this intervention.
12. BLACK WIDOW SPIDER BITES Found throughout US & worldwide
�Red hourglass�
Neurotoxic venom
Pain but NO necrosis
Abdominal rigidity
Rx = antivenom
The black widow spider has a potent neurotoxic venom and is considered the most venomous spider in North America.
This spider is found worldwide and five species occur within the US. The female spider is usually the culprit of bites.
You can distinguish this spider by its shiny black color and characteristic �red hourglass� design on the its underside.
The spider injects its prey with a very potent venom -- however, the female injects such a small dose of venom that it rarely causes death. Reports indicate human mortality at well less than 1% from black widow spider bites.
Unlike the bite of the brown recluse spider, there is NO necrosis or conspicuous swelling of the skin
The venom travels in the bloodstream throughout the body and acts on the nervous system, causing varying degrees of pain.
Severe muscle pain and cramps may develop in the first two hours and are usually first felt in the back, shoulders, abdomen and thighs.
Other symptoms include weakness, sweating, headache, anxiety, itching, nausea, vomiting, difficult breathing and increased blood pressure. Young children, the elderly and those with high blood pressure are at highest risk of developing symptoms from a black widow spider bite.
Symptoms often diminish after a day or so and cease after several days. Serious long-term complications or death are very rare.
There is an antivenom available for black widow spider bites and it has been effective in reducing the number of deaths
http://en.wikipedia.org/wiki/Image:Black_Widow_11-06.jpg
http://www.calpoison.org/public/spiders.htmlThe black widow spider has a potent neurotoxic venom and is considered the most venomous spider in North America.
This spider is found worldwide and five species occur within the US. The female spider is usually the culprit of bites.
You can distinguish this spider by its shiny black color and characteristic �red hourglass� design on the its underside.
The spider injects its prey with a very potent venom -- however, the female injects such a small dose of venom that it rarely causes death. Reports indicate human mortality at well less than 1% from black widow spider bites.
Unlike the bite of the brown recluse spider, there is NO necrosis or conspicuous swelling of the skin
The venom travels in the bloodstream throughout the body and acts on the nervous system, causing varying degrees of pain.
Severe muscle pain and cramps may develop in the first two hours and are usually first felt in the back, shoulders, abdomen and thighs.
Other symptoms include weakness, sweating, headache, anxiety, itching, nausea, vomiting, difficult breathing and increased blood pressure. Young children, the elderly and those with high blood pressure are at highest risk of developing symptoms from a black widow spider bite.
Symptoms often diminish after a day or so and cease after several days. Serious long-term complications or death are very rare.
There is an antivenom available for black widow spider bites and it has been effective in reducing the number of deaths
http://en.wikipedia.org/wiki/Image:Black_Widow_11-06.jpg
http://www.calpoison.org/public/spiders.html
13. OTHER ARTHROPODS DIRECTLY CAUSING DISEASE Allergic reactions
Bites/Stings
Dust mites/Cockroaches
Myiasis
14. ARTHROPODS AS VECTORS From the perspective of infectious diseases, vectors are the transmitters of disease-causing organisms � they carry the pathogens from one host to another. Vectors are usually considered to be arthropods.
But, keep in mind that non-arthropods, such as foxes, raccoons, and skunks, can also act as disease vectors
http://www.enotes.com/public-health-encyclopedia/vector-borne-diseasesFrom the perspective of infectious diseases, vectors are the transmitters of disease-causing organisms � they carry the pathogens from one host to another. Vectors are usually considered to be arthropods.
But, keep in mind that non-arthropods, such as foxes, raccoons, and skunks, can also act as disease vectors
http://www.enotes.com/public-health-encyclopedia/vector-borne-diseases
15. VECTOR-BORNE DISEASES
MAJOR VECTORS:
MOSQUITOS
TICKS
FLEAS
Several genera of arthropods play a role in human disease, but mosquitoes and ticks are the most notable disease vectors.
The most significant mode of vector-borne disease transmission is by biological transmission by blood-feeding arthropods. The pathogen multiplies within the arthropod vector and is transmitted when the arthropod takes a blood meal.
Mechanical transmission of disease agents may also occur when arthropods physically carry pathogens from one place or host to another, usually on body parts.
http://www.enotes.com/public-health-encyclopedia/vector-borne-diseasesSeveral genera of arthropods play a role in human disease, but mosquitoes and ticks are the most notable disease vectors.
The most significant mode of vector-borne disease transmission is by biological transmission by blood-feeding arthropods. The pathogen multiplies within the arthropod vector and is transmitted when the arthropod takes a blood meal.
Mechanical transmission of disease agents may also occur when arthropods physically carry pathogens from one place or host to another, usually on body parts.
http://www.enotes.com/public-health-encyclopedia/vector-borne-diseases
16. MOSQUITO-BORNE DISEASES First, we�ll look at the mosquito-borne diseases.First, we�ll look at the mosquito-borne diseases.
17. DENGUE FEVER Dengue virus is a flavivirus Transmitted by aedes mosquitoes Composed of single-stranded RNA Has 4 serotypes (DEN-1, 2, 3, 4)