Download
1 / 14
140 likes | 445 Views
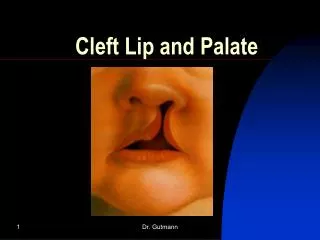
PROBLEMS IN CLEFT LIP AND PALATE (CLP). Congenital anomalies Feeding Hearing Speech Disruption of facial growth Disruption of dental development Dental anomalies Psychosocial.

E N D
Congenital anomalies Feeding Hearing Speech Disruption of facial growth Disruption of dental development Dental anomalies Psychosocial
Disturbances in dental and skeletal development caused by the clefting process itself depend upon the site an severity of the cleft • Lip only • there’s lil effect in this type, although notching of the alveolus adjacent to the cleft lip may sometimes be seen. • Lip and alveolus • Unilateral cleft lip and alveolus unsually associated with segmental displacement. • Bilateral casese the premaxilla may be rotated forwards. • Lat inc on the affected side may exhibit • Congenital absence • An abnormality of tooth size and/or shape • Enamel defect • Two conical teeth, one on each side of the cleft
Lip and Palate • In unilateral cleft rotation and collapse of both segments inwards anteriorly is usually seen( on the affected side) • In bilateral clefts both lateral segments are often collapsed behind a prominent premaxilla • Palate only • A widening of the arch post[usually] • Cleft pt has more concave profile & a degree of this is d/t a restriction of growth. • Pt tends to have more retrognathic maxilla & mand & reduced upper face height
Babies with cleft palates can swallow once the material being fed reaches hypopharynx Have extreme difficulty producing negative pressure in their mouth to allow sucking. Overcome by use of specially designed large syringes with rubber extension tubes connected to them or use of obturator.
Speech development is adversely affected by the presence of fistulae in the palate and by velopharyngeal insufficiency (where the soft palate is not able to make an adequate contact with the back of the pharynx to close off the nasal airway). A cleft involving the posterior part of the hard and soft palate will also involve the tensor palati muscles. which act on the Eustachian tube. This predisposes the patient to problems with middle-ear ventilation (known colloquially as 'glue ear'). Obviously, hearing difficulties will also retard a child's speech development. Therefore management of the child with a cleft involving the posterior palate must include audiological assessments and myringotomy with or without grommets as indicated.
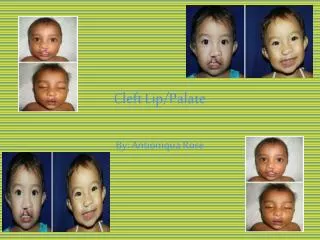
Individuals with unoperated clefts • they do not experience significant restriction of facial growth, although there is a lack of development in the region of the cleft itself, possibly because of hypoplasia. • Individuals who have undergone surgical repair to CLP • exhibit marked restriction of mid-face growth anteroposteriorly (maxillary retrusion) and transversely. • This is attributed to the restraining effects of the scar tissue , which result from surgical intervention.
Cleft affecting the alveolus result in non-eruption or displacement of lateral incisors or canines. Bilateral cleft premaxilla (prolabium) is displaced along with the incisors.
Delayed eruption (delays increases with severity of cleft) Hypodontia General reduction in tooth size.eg;microdontia Abnormalities of tooth size and shape. Enamel defects.eg;hypomineralized Impacted teeth (maxillary canines) Missing teeth Supernumerary tooth
Space maintenance and control is instituted during childhood. Appliances to maintain or increase the width of dental arch are frequently used. This treatment is usually begin with eruption of the first maxillary permanent molars. Comprehensive orthodontic care is deferred until later, when most of permanent teeth erupted. Consideration of orthognathic surgical intervention for skeletal discrepancies and malocclusion.
Poor self image Lack of self confience