Download
1 / 32
• 390 likes • 1.11k Views
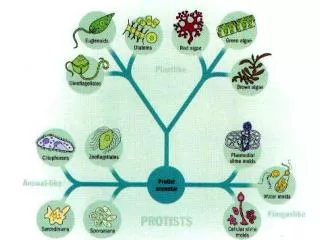
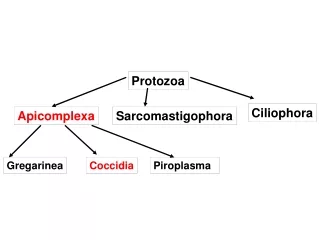
Intestinal Protozoa. Mark F. Wiser Department of Tropical Medicine. Flagellates : Giardia lamblia Dientamoeba fragilis Chilomastix mesnili Trichomonas hominis Enteromonas hominis Retortamonas intestinalis Ameba : Entamoeba histolytica Entamoeba dispar Entamoeba coli

E N D
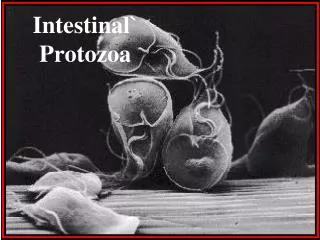
Intestinal Protozoa Mark F. Wiser Department of Tropical Medicine
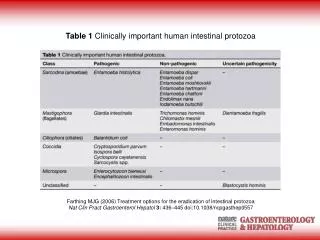
Flagellates: • Giardia lamblia • Dientamoeba fragilis • Chilomastix mesnili • Trichomonas hominis • Enteromonas hominis • Retortamonas intestinalis • Ameba: • Entamoeba histolytica • Entamoeba dispar • Entamoeba coli • Entamoeba hartmanni • Endolimax nana • Iodamoeba bütschlii • Apicomplexa: • Cryptosporidium hominis • Cryptosporidium parvum • Cyclospora cayetanensis • Isospora belli • Other: • Blastocystis hominis • Balantidium coli INTESTINAL PROTOZOA unicellular eukaryotic organisms
Fecal-Oral Transmission Factors • poor personal hygiene • food handlers • institutions • children in day care centers • developing countries • highly endemic • poor sanitation • travelers diarrhea • water-borne epidemics • male homosexuality • oral-anal contact • zoonosis • Entamoeba = no • Cryptosporidium = yes • Giardia = controversial • Control/Prevention • improve personal hygiene • especially institutions • treat asymptomatic carriers • eg, family members • health education • hand-washing • sanitation • food handling • protect water supply • treat water if questionable • boiling • iodine • not chlorine
Giardia lamblia • worldwide distribution • higher prevalence in developing countries (20%) • 1-6% in temperate countries • most common protozoa found in stools • ~200 million clinical cases/year • giardiasis • often asymptomatic • acute or chronic diarrhea • fecal-oral life cycle • CYST • infective stage • passed in feces • TROPHOZOITE • replicative stage • small intestine
Clinical Features and Symptoms • Subacute/Chronic • recurrent diarrheal episodes • cramps uncommon • sulfuric belching, ano-rexia, nausea frequent • can lead to weight loss and failure to thrive • Range of Outcomes • asymptomatic/latent • acute short-lasting diarrhea • chronic/nutritional disorders • Acute Symptoms • 1-2 week incubation • sudden explosive, watery diarrhea • bulky, frothy, greasy, foul-smelling stools • no blood or mucus • upper gastro-intestinal uneasiness, bloating, flatulence, belching, cramps, nausea, vomiting, anorexia • usually clears spontaneously (undiagnosed), but can persist or become chronic
Pathogenesis • epithelial damage • villus blunting • crypt cell hypertrophy • cellular infiltration • malabsorbtion • enzyme deficiencies • lactase (lactose intolerance) • Possible Mechanisms • mechanical irritation • obstruction of absorption
cyst trophozoite Entamoeba histolytica • cosmopolitan distribution • worldwide incidence: 0.2-50% • no animal reservoirs • typical fecal-oral life cycle • inhabits large intestine • facultative virulent pathogen • estimated 50 million cases/year • 100,000 deaths/year • Entamoeba dispar • morphologically identical • non-pathogenic
Pathogenesis of Amebiasis • NON-INVASIVE • ameba colony on intestinal mucosa • asymptomatic cyst passer • non-dysenteric diarrhea, abdominal cramps, other GI symptoms • INVASIVE • necrosis of mucosa ulcers, dysentery • ulcer enlargement dysentery, peritonitis • metastasis extraintestinal amebiasis • cessation of cyst production
ulcers with raised borders • little inflammation between lesions
‘flasked-shaped ulcer’ • trophozoites at boundary of necrotic and healthy tissue • trophozoites ingesting host cells • dysentery (blood and mucus in feces)
Ulcer Enlargement and Disease Progression • ameba expand laterally and downward into lamina propria • localized sloughing (ulcers coalesce) • perforation of intestinal wall • peritonitis • 2o bacterial infections • local abscesses • ameboma (=amebic granuloma) ameboma = inflammatory thickening of intestinal wall around the abscess (can be confused with tumor)
Extraintestinal Amebiasis • metastasis via blood stream • primarily liver (portal vein) • other sites less frequent • ameba-free stools common • high antibody titers
Amebic Liver Abscess • chocolate-colored ‘pus’ • necrotic material • usually bacteria free • lesions expand and coalesce • further metastasis, direct extension or fistula
Pulmonary Amebiasis • rarely primary • rupture of liver abscess through diaphragm • 2o bacterial infections common • fever, cough, dyspnea, pain, vomica • Cutaneous Amebiasis • intestinal or hepatic fistula • mucosa bathed in fluids containing trophozoites • perianal ulcers • urogenital (eg, labia, vagina, penis)
Facultative Pathogenicity • 85-90% of infected individuals are asymptomatic • ~10% of the symptomatic will develop severe invasive disease
Molecular Epidemiology • molecular probes used to survey for E. dispar and E. histolytica • E. dispar ~10-fold > E. histolytica • discrete endemic pockets of E. histolytica • many asymptomatic E.h. infections • ~10% of the E.h. infections are associated with invasive amebiasis • ~25% seropositive for E. histolytica in endemic areas
a pathogen has an inherent ability to break host cell barriers • virulence usually correlates with ability to replicate within host • various degrees of virulence may be exhibited depending on conditions
penetration of mucus layer • contact-dependent killing of epithelial cells • breakdown of tissues (extracellular matrix) • contact-dependent killing of neutrophils, leukocytes, etc.
Cryptosporidium • fecal-oral transmission (coccidian type life cycle) • two species infecting humans • C. parvum: cattle and other mammals • C. hominis: only humans • first human case reported in 1976 • initially believed to be rare and exotic • now known to be common human pathogen • self-limiting diarrhea in immunocompetent persons • profuse, watery diarrhea associated with AIDS (life threatening)
Cryptosporidium Life Cycle • Infectious form = oocyst • Sporozoites ‘invade’ intestinal epithelial cells • Merogony • produce merozoites • Gametogony • produce micro- and macrogametes • Sporogony • produce sporozoites • completed on host cell • thin (autoinfection) or thick walled oocysts
Molecular Epidemiology • 2 major genotypes identified: • genotype 1 (C. hominis) • only human sources • non-infective for mice or calves • anthroponotic transmission • genotype 2 (C. parvum) • human and bovine sources • infective for mice and calves • zoonotic transmission • other genotypes (eg, C. felis, dog type, etc) rare • isolated only from AIDS patients
Modified from Graczyk et al, Parasitol. Today 13:348 (1997) Water Borne Outbreaks of Cryptosporidiosis in the USA • Human Cryptosporidiosis • epidemic diarrhea in institutions and hospitals • highly transmissible (19% household members)
The Milwaukee Outbreak NEJM 331:161 (1994) • massive cryptosporidiosis outbreak following spring thaw • >400,000 people may have been affected • based on clinical symptoms (acute watery diarrhea) • ~100-fold higher prevalence of Cryptosporidium oocysts in stools than normal • other enterics (including Giardia, bacteria, viruses) were at ~normal levels • treated water had high levels of turbidity 3/23-4/5/1993 • oocysts identified in ice made during this period
Symptoms of 205 patients with Confirmed Cases of Cryptosporidiosis During the Milwaukee Outbreak
Pathogenesis • enterocytes damaged or killed • villus atrophy (blunting) • Na+ absorption • intercellular permeability • crypt cell hyperplasia • Cl- secretion • inflammation in lamina propria • cytokines and neurohormones? • enhanced secretion of antibodies (IgA)? • DIARRHEA • enterocyte malfunction (osmotic) • impaired absorption • enhanced secretion • inflammatory diarrhea • mucosal invasion • leukocytes in stools • secretory diarrhea • toxin associated • watery
Diagnosis of Intestinal Protozoa • suspect: acute or chronic GI symptoms • confirmed: detection of parasite in feces • copro-antigens or molecular probes • Cryptosporidium • acid-fast stain • Giardia • 3 non-consecutive days (inconsistent excretion) • duoenal aspirates or biopsy • presumptive treatment in chronic cases • Entamoeba • histolytica vs dispar • sigmoidoscopy (lesions, aspirates, biopsy) • extra-intestinal disease
Diagnosis of Extraintestinal Disease • symptoms associated with specific organ • history of dysentery • hepatic • right upper quadrant pain • enlarged liver • serology (current or past?) • imaging (CT, MRI, ultrasound) • abscess aspiration • only select cases • reddish brown liquid • trophozoites at abscess wall
Treatment Cryptosporidium Giardia Entamoeba • Drug of Choice • metronidazole (Flagyl) • 750 mg/tid/5d • >90% cure rate • Alternatives • tinidazole (single dose) • paromomycin (pregnancy) • quinicrine • furazolidone • asymptomatic • iodoquinol or paromomycin • symptomatic • metronidazole or tinidazole • followed by lumenal agents • drain liver abscess • only with high probability of rupture! • no highly effective drugs • paromomycin has modest benefit • supportive care • rehydration • nutritional support • anti-motility agents