Download
1 / 40
480 likes | 1.87k Views
INTESTINAL & LUMINAL PROTOZOA. Dr Ekta Chourasia Lecturer, Microbiology. Algorithm. Name of the parasite. Disease caused. System/s affected. Forms of the parasite. Life cycle: Definitive host, intermediate host. Site of localization. Infective form. Mode of transmission.

E N D
INTESTINAL & LUMINAL PROTOZOA Dr Ekta Chourasia Lecturer, Microbiology
Algorithm Name of the parasite Disease caused System/s affected Forms of the parasite Life cycle: Definitive host, intermediate host Site of localization Infective form Mode of transmission Signs & symptoms Laboratory diagnosis Treatment & Prevention Dr Ekta,Microbiology
Phylum PROTOZOA • Definition – A microscopic unicellular organism which is morphologically and functionally complete i.e. a single cell can perform all the functions like reproduction, respiration, digestion, excretion, etc. • Morphology – Cytoplasm & Nucleus • Cytoplasm – divided into • Ectoplasm: protective, locomotive (pseudopodia, cilia & flagella) & sensory function • Endoplasm: nutritive & reproductive function. Dr Ekta,Microbiology
Taxonomy Kingdom Animalia Subkingdom Protozoa Phylum Sarcomastigophora Subphylum Sarcodina amoeba Entamoeba, Nagleria Subphylum Mastigophora Giardia, Trichomonas, (Flagellates) Trypanosoma, Leishmania Phylum Apicomplexa Plasmodium, (Sporozoa) Toxoplasma, Cryptosporidium, Isospora Phylum Ciliophora (ciliates)Balantidium Phylum Microspora Microsporidium Dr Ekta,Microbiology
Ecological Niches in the Human Body • Skin Leishmania • Eye Acanthamoeba • Mouth Amoebae and flagellates (usually non - pathogenic) • Gut Entamoeba (and invasion to liver), Giardia, Cryptosporidium, Isospora, Balantidium • G.U. tract Trichomonas Dr Ekta,Microbiology
Ecological Niches in the Human Body • Bloodstream Plasmodium, Trypanosoma • Spleen Leishmania • Liver Leishmania, Entamoeba • Muscle Trypanosoma cruzi • CNS Trypanosoma, Naegleria, Toxoplasma, Plasmodium Dr Ekta,Microbiology
Protozoa – Intestinal & Luminal Pathogenic Amoeba Entamoeba histolytica Amoebiasis (Dysentry & soft tissue abscesses) Giardia lamblia Giardiasis (malabsorbtion) Flagellates Trichomonas vaginalis Vaginitis Ciliates Balantidium coli Diarrhoea Free living amoeba Meningoencephalitis & Keratitis Acanthamoeba Naeglaria Primary Meningoencephalitis Dr Ekta,Microbiology
Blood Protozoa Plasmodium Malaria Leishmania Leishmaniasis (Visceral, Cutaneous) Trypanasoma African sleeping sickness, Chagas disease Toxoplasma gondii Toxoplasmosis (congenital infections) Dr Ekta,Microbiology
Pathogenic Entamoeba histolytica Balantidium coli Giardia lamblia Cryptosporidium parvum Cyclospora cayetanensis Isospora belli Microsporidia Commensal/ Non-pathogenic Entamoeba coli Entamoeba hartmanii Iodamoeba bütschlii Dientamoeba fragilis Intestinal Protozoa Dr Ekta,Microbiology
Case • A 28 year old male presented with low grade fever, loss of appetite and pain in right upperquadrant since 15 days. • Three months back, he suffered from dysentery. • Physical examination revealed an enlarged liver • Blood picture showed leucocytosis with raised eosinophils. • CT scan showed the presence of cavitatory lesion in the right side of the liver. • Aspirate from liver showed motile trophozoites in wet mount preparation. Dr Ekta,Microbiology
Entamoeba histolytica • Habitat – large intestine (mucosa & submucosa) • Morphological forms – • Trophozoite - ameboid shape, 15-30µ in diameter, motile form • Cyst - spherical, 12-15µ, the cytoplasm contains dark staining chromatoid bodies and 1 to 4 nuclei with a central karyosome, infective form, non motile. • Disease - Amoebiasis. Dr Ekta,Microbiology
Methods of Reproduction • Excystation – process of transformation of cysts totrophozoites that occurs only with the entry of cyst in thealimentary canal of man. Each cyst gives rise to eight amoebulae. One amoebule – one trophozoite. • Encystation – process of transformation of trophozoites tocysts, occurs in the lumen of large intestine of an infected individual. * cysts never seen in tissues of man • Multiplication – by binary fission, occurs only in trophozoite phase (inside tissues) Dr Ekta,Microbiology
Epidemiology: Amoebiasis • Man is the commonest source of infection • Infective form: Mature quadrinucleate cyst • Mode of infection: feco-oral route by ingestion of food & drink contaminated with cyst. - food handling by infected individuals /carriers (contact / convalescent carriers) - houseflies • Incubation period: 4-5 days Dr Ekta,Microbiology
Life cycle of E. histolytica Dr Ekta,Microbiology
Pathogenicity of Entamoeba histolytica • Amoebiasis – all clinical conditions produced by E. histolytica in human host. • Pathogenic lesions – two types: • Primary or intestinal lesions – confined to large intestine • Secondary or metastatic lesions (extraintestinal) – due to migration of trophozoites to liver, lungs & brain. Dr Ekta,Microbiology
Amoebiasis • Acute amoebic dysentery - Frequent dysentery with necrotic mucosa and abdominal pain: flask shaped ulcers in colonic mucosa • Extraintestinal amoebiasis – liver (amoebic liver abscess), lung & brain abscess • Asymptomatic carrier state • Amoeboma – granulomatous tumour like growth. Dr Ekta,Microbiology
Amoebic v/s bacillary dysentery Dr Ekta,Microbiology
Amoebic liver abscess • About 2 to 10% suffer from hepatic complications • Generally appears about one to three months after the disappearance of dysentery • Trophozoites are carried to the liver via portal vein • Multiplication of trophozoites – obstruction to circulation – thrombosis of sinusoids – necrosis of surrounding liver cells – formation of liver abscess begins – liquefaction of centre of abscess (cytolysis – pus). • Trophozoites can be seen in the peripheral zone of abscess. • Pus “anchovy sauce pus” – mixture of sloughed liver tissue & blood, chocolate brown in colour, thick in consistency. Dr Ekta,Microbiology
Complications of Amoebic Liver Abscess • Rupture of abscess: • Externally • Internally into • Right pleural cavity • Right lung • Peritoneal cavity • Below diaphragm – subphrenic abscess • Metastasis – lungs, brain, skin, spleen Dr Ekta,Microbiology
Laboratory diagnosis - Amoebiasis Type Intestinal Extraintestinal / Hepatic Stool Liver aspirate / stool Specimen (Anchovysauce pus) Microscopy Trophozoites / Cysts Only trophozoites Dr Ekta,Microbiology
Laboratory diagnosis - Microscopy • Stool Examination – saline & stained preparation • Saline – motile trophozoites with ingested RBCs • Iodine – body stains yellow, nucleus with a central karyosome, brown glycogen mass. • Fixed & stained - HE Dr Ekta,Microbiology
Laboratory diagnosis • Culture – special medium TYIS-33 supports the growth of E. histolytica • Serological tests – detection of anti-amoebic antibodies in invasive amoebiasis (latexagglutination), Ag detection in feces by ELISA • results become negative after cure • Detection of asymptomatic carrier – cyst in feces, at least three stool specimen Dr Ekta,Microbiology
Treatment & Prevention • Treatment – • Tissue & luminal - Metronidazole / Tinidazole • Prevention • Personal hygiene • Safe drinking water • Protection of food & water from contamination • Avoid use of raw vegetables & fruits Dr Ekta,Microbiology
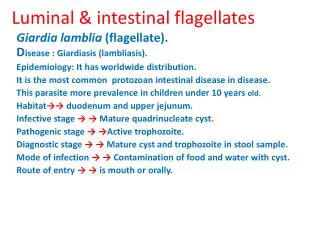
Giardia lamblia • Habitat: duodenum & upper jejunum • Morphology: two forms • Trophozoite – tennis racket shaped, dorsal surface convex, ventral surface concave with sucking disc (falling leaf motility) • Cyst – oval, diagonal axostyles Dr Ekta,Microbiology
Falling Leaf motility Dr Ekta,Microbiology
Life Cycle - Giardiasis Large intestine: encyst Infective form: Cysts Steatorrhoea Ingestion: Faeco-oral Mucus Diarrhoea Stomach: Resist acid Abnormal villous architecture Small Intestine - excyst Binds to mucosa by ventral sucking disc No invasion - submucosa Dr Ekta,Microbiology
Laboratory diagnosis - Giardiasis Specimens: Stool, duodenal aspiration Gelatin capsules: Enterotest Microscopy: Trophozoites / cysts Treatment: Metronidazole / Tinidazole Prevention: Personal hygiene, avoid food & water contamination, drink safe water Dr Ekta,Microbiology
Balantidium Coli Largest protozoal parasite of humans Habitat: Large intestine Morphological Forms: Trophozoite: (60-70µ) Ovoid shape, moves by cilia Kidney shape macro-nucleus, round micronucleus Motile - rotatory Cyst: (40-50µ) Ovoid, macronucleus Dr Ekta,Microbiology
Life Cycle – B coli Infective form: Cysts Mucosal & submucosal ulcers No extra intestinal invasion Ingestion: Faeco-oral Stomach: Resist acid Diarrhoea / Dysentery Large intestine: encyst Small Intestine - excyst Passed out in feces Large intestine – trophozoites (one cyst – one trophozoite) Dr Ekta,Microbiology
Laboratory diagnosis Specimen: Stool Diarrhoeic- trophozoites, formed - cysts Microscopy: Trophozoites / cysts Tetracycline 500mg four times a day for 10 days Metronidazole / tinidazole also effective Treatment: Prevention: Personal hygiene, avoid food & water contamination, drink safe water Dr Ekta,Microbiology
Trichomonas vaginalis No cyst form Only trophozoite form Sexually transmitted disease Men are usually asymptomatic Females Vaginitis Purulent discharge Diagnosis Demonstration of trophozoites in wet films / giemsa stained smear Treatment Metronidazole Dr Ekta,Microbiology
Amebic Meingoencephalitis Amoeba is found in lakes, enters organisms through nasal passageways. Lethal destruction of CNS. Dr Ekta,Microbiology
Free living amoeba - Naegleria fowleri Disease Primary amoebic meningoencephalitis (PAM) Forms Amoeba, cyst, flagellated trophozoite Swimming – nose – olfactory epithelium – cribriform plates- cerebral cortex – hemorrahge & necrosis Pathogenicity Lab diagnosis Amoeboid form in CSF / never cysts Amphotericin B / Rifampin Treatment Chlorine level at or above 0.5 mg/L Prevention Dr Ekta,Microbiology
Free living amoeba - Acanthamoeba Diseases Granulomatous amoebic meningoencephalitis (GAE) Amoebic Keratitis Forms Amoeba, cyst, No flagellated trophozoite Pathogenicity Immunocompromised – lungs / abrasions – blood – brain. Keratitis: contact lens – trauma / nonsterile wash solution Lab diagnosis Amoeboid form / cyst in CSF or corneal scrapings GAE - Amphotericin B Treatment Keratitis - Propamidine with neomycin Dr Ekta,Microbiology
SUMMARY Dr Ekta,Microbiology