Download
1 / 28
280 likes | 524 Views
Establishing a Need for Comprehensive Interventions: Issues with Professional Training and Practice. . . Extreme competition Difficult decisions Lack of limits Suppressed emotions Operating a business Living up to the position Lack of balance Adversarial nature of

E N D
1. TREATING DISRUPTIVE BEHAVIOR IN PHYSICIANS Alexis Polles, MD
Philip Hemphill, LCSW
Professional Enhancement Program
Hattiesburg, MS
601-288-4772
apolles@forrestgeneral.com
2. Establishing a Need for Comprehensive Interventions: Issues with Professional Training and Practice
3. OBJECTIVES To identify warning signs of individuals whom may be at increased risk for disruptive workplace behavior
To explore the impact of disruptive behavior on organizations and develop strategies for managing the physician and employees affected within the workplace
To understand the components of a multi-modal approach for physicians with disruptive behavior which integrates biological, psychological, systemic, and addictive interventions
4. Defining the Term The term disruptive physician� applies to physicians who exhibit behavior that �interferes with patient care or could reasonably be expected to interfere with the process of delivering quality care.�
5. Disruptive Physician Behavior JC adopted this issue as a National Patient Safety Goal for 2007. This requires that physician behavior that is destabilizing patient care be addressed. This creates both an opportunity and a challenge. (Wardrop, 2006)
Closely linked to an organization�s culture
6. Creating and Maintaining a Culture of Safety Setting expectations for behavior
Working in teams
Respecting self and others
Code of Conduct for all hospital workers
Education
Free online program from Texas Med. Assoc. (charge for CME credit)
Define desirable behaviors
Incident Reports
Created by any person, employee, practitioner, patient, or visitor who observes disruptive behavior
JC standards says policy includes disruptive behavior by �ANYONE� who works in the organization. (e.g. board members, management, volunteers, clinical staff, etc.)
7. Hospital�s Perspective When a physician�s conduct:
disrupts the operation of the hospital
affects the ability of others to get their jobs done
creates a �hostile work environment� for hospital employees or other physicians on the medical staff
begins to interfere with the physician�s own ability to practice competently
One court has held that hospitals have a duty to take action in such situations.
8. Counter Point Abuse of the disruptive physician clause
The term �disruptive� is vague and subjective
Allowed by non-vigilant physicians who did not seek legal advice on bylaws changes urges by hospital administrators
Part of strategic plan developed in 1990 by the hospital industry with the goal of gaining more control of physicians in hospitals
9. MEMO TO THE DISRUPTIVE PHYSICIAN: Oh how we strive for quality high,
For health and most of all safety.
But a word to the wise; reproof we despise
And outspoken physicians; We hate thee
Feel free to opine, but note we define
All critics as never constructive.
And, thus shall ensue a sham peer review
And henceforth you�re labeled �disruptive�
10. Behavior Outcomes: Nurses and Physicians Follow-up survey to one that examined Nurse/Physician relationships and their impact on nursing satisfaction and retention
50 VHA hospitals participated with 1500 participants
Nurses disruption nearly as frequent as physicians
Behavior impacts general stress and workplace relationships
But more importantly results in adverse events, medical errors, patient safety, patient mortality, quality of care, and patient satisfaction.
Thus consequences go beyond nurses� job satisfaction
11. Respondents (Nurses, Physicians, and Administrators) Who Witnessed Disruptive Behavior in Physicians and Nurses
12. Respondents� Answers to Selected Survey Questions
13. SCOPE OF THE PROBLEM Survey by the ACPE (n=1600)
95% reported encountering these behaviors on a regular basis
1 in 3 said they observe problems with physician behavior either weekly or monthly
(Keogh & Martin, 2004)
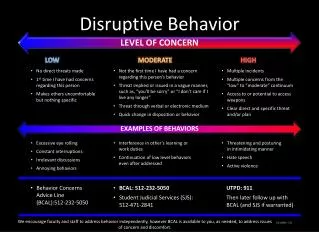
14. Breakdown of typical problems Refusal to complete tasks or carry out duties 52%
Physical abuse (includes throwing items) 9%
Insults 37%
Disrespect 83%
Yelling 41%
Other 13.5%
15. Summary All of the behaviors involve inappropriate and indirect communications.
�Communication failures are the leading cause of inadvertent patient harm�
(Leonard, et al, The human factor: the critical importance of effective teamwork and communication in providing safe care. Quality Safe Health Care 2004; 13
16. Why is a diagnosis important? �Should a physician�s disruptive behavior reflect a health problem, the JC standards go further to require the medical staff to implement a process to identify and manage the individual physician�s health-related matters� disruptive behavior may be reasonably interpreted to require anger and/or stress management or formal behavioral counseling and monitoring.�
17. Level of Care Determinations Follow by-laws
Assessment (local or specialized)
No further treatment needed
Assessment and structured monitoring
Outpatient individual and/or group work
Intensive profession specific focused work
Cognitive Behavioral
Educational
Psychodynamic
Addictions focused
Retirement from practice / suspension or revocation of license
20. GOOD LIVES MODEL What this means is that it is not enough to simply equip individuals with skills to control or manage their risk factors, it is imperative that we also give the opportunity to fashion a more adaptive personal identity, one that bestows a sense of meaning and fulfillment (Maruna, 2001).
21. Intensive Residential This physician was referred for disruptive workplace behavior in 2 separate hospitals, though more pronounced at one, as evidenced by angry and belittling behavior toward staff (particularly subordinates).
Four years earlier, he was evaluated for anger issues and was followed by an outpatient therapist. Shortly after that evaluation, he entered into a contract with the state monitoring board at the request of the hospital.
He was an only child with no issues of abuse. There was no evidence of inappropriate anger in social or religious settings.
The only significant family history was maternal grandmother with grief following death of her spouse.
Presented as overly cautious with a defensive profile, reluctant to disclose much, and concerned about making a good impression.
22. RESULTS Collateral information
Described as hostile, argumentative, and demeaning.
Sources stated �if anything goes wrong he finds someone to blame�his response is out of proportion and his behavior is out of control.�
Another said, �it was just awful, it was ugly, he was pounding the counter enraged and calling another physician �stupid��.
A third said �he looked like a psychotic patient fleeing from the psych ward.�
Some felt he was dishonest while others thought he tried to prove himself by being the best surgeon and making the most money.
Our recommendations were that he enter an intensive, structured treatment program to deal with narcissistic personality disorder and disruptive workplace behavior.
23. Data from Consecutive Admissions from 10/1/02 to 10/31/07
Total Admissions: 355
Males 282 79%
Female 73 21%
Average Age 46
Average # Tx Days 44
Physicians 163 46%
Pharmacists 15 4%
Dentists 11 3%
Nurses 6 1%
Physician Assistants 3 1%
Veterinarians 2 1%
Other Professionals 156 44%
24. Most Common Axis I and Axis II Diagnosis AXIS I (n=160)
Drug Abuse/Dep. 64%
Alcohol Abuse/Dep. 34%
Depressive Disorders 34%
Anxiety Disorders 26%
Psychosexual Disorders 13%
Bipolar Disorders 11%
Eating Disorders 8%
Intermittent Explosive Disorders 2%
Other 55%
AXIS II (Personality DO and traits) (n=90)
Narcissistic 34%
Obsessive Compulsive 18%
Pers. Disorder, NOS 16%
Paranoid 11%
Histrionic 11%
Avoidant 10%
Antisocial 8%
Dependent 8%
Borderline 2% Some of the most common Axis I Disorders found during our evaluations
Axis II diagnosis percentages includes those diagnosed with either the Personality Disorder or the traits.Some of the most common Axis I Disorders found during our evaluations
Axis II diagnosis percentages includes those diagnosed with either the Personality Disorder or the traits.
25. On-site visit for treatment participants prior to discharge provides feedback.
Self, staff, peers, and supervisors complete an anonymous survey.
Online survey is completed on a quarterly basis.
Feedback report is provided to monitoring program, ratee, supervisor, and other relevant parties (e.g., psychiatrist, physician executives, PHP, therapist).
26. Highlights need to collect data from multiple sources
Discrepancy between staff, peer, supervisor, and self ratings.
Feedback provides roadmap for behavior change
Some people work with therapists to make changes.
Return visit to treatment helpful
Initial months of monitoring typically display no significantly disruptive behavior�..but, after a few months patterns begin to show.
27. 33 questions
28 Likert-type questions regarding ratee�s behavior
1 question concerning how many hours rater works with ratee
1 question about the rater�s title
3 open-ended questions that solicit comments
29. Professionals exhibiting disruptive behavior in the workplace require intensive specialized interventions.
Many can make positive, lasting changes by utilizing an approach that is consistent during the evaluation, treatment and monitoring phases of care.